
What are the Pros and Cons of Each Type of Vaccine?
Story at a Glance:
•The vaccine industry has been largely shielded from scrutiny because of the belief “vaccines are safe and effective.” As a result, there is very little discussion of how vaccines are made, or the merits of each approach. Here, I will review some of the foundational principles of vaccine design and the clinical implications of those designs that I believe are critical to understanding their efficacy.
•For example, hot lots (poorly produced dangerous batches i.e. “toxic medicine”) are an inevitable consequence of the production methods used for many types of vaccines, and over the years there have been dozens (if not more) of disasters that have been covered up, but nonetheless frequently led to many vaccines being withdrawn from the market. If the potential of hot lots emerging had been known by the medical field, physicians in practice likely would have been able to recognize when hot vaccine lots were being released onto the market and the tsunami of deaths they caused could have been averted.
•Likewise, the principles of vaccine design are also critical for parents trying to decide which immunizations are appropriate or inappropriate for their children to receive (as the relative risks of each type vary immensely).
•Finally, I will cover what I believe to be the safest and most effective approaches to vaccination that have been developed. These include relatively unknown and affordable approaches that perform better than vaccination (both for halting epidemics spreading through a country or to protect individual children from common childhood illnesses) and which ones can be used to therapeutically treat a variety of debilitating chronic illnesses (e.g., Lyme disease, chronic fatigue, rheumatoid arthritis alongside a variety of other immunologic or allergic conditions).
Note: in the last 24 hours I have received a lot of requests to comment on the recent assassination attempt. Shortly after the events, I did my best to provide a few unique perspectives on the events which can be viewed here, and presently has received over 300k views.
I believe the most effective marketing slogan in history was “Vaccines are safe and effective.” This is because it implies 100% safety and 100% efficacy (which is impossible regardless of the therapy) but simultaneously avoids explicitly committing to that claim. Thus, the product is zealously promoted by its supporters but simultaneously escapes accountability for its continual failures (as no concrete promise is ever broken each time the vaccine is shown to be unsafe or ineffective).
One of the less appreciated consequences of this slogan (“safe and effective”) is that it causes most people to view all vaccines as being equivalent to each other, when in reality they are very different. For example, there have now been multiple high profile admissions that if the mRNA injections had been marketed as “gene therapies” almost no one would have taken them, but since they were instead presented to the public as “vaccines” they were exuberantly taken up across the globe.
In my eyes, one of the few upsides to the COVID-19 vaccine tragedy has been that the scale of harm the vaccines have caused has made the public begin questioning many of the lies that have been used to sell the vaccines to us for decades. For example, at a recent Congressional, in an attempt to escape culpability for a previous lie he’d made, Fauci stated that “I don’t believe any vaccine is 100% effective” and hence dispelled the cloak of ambiguity which has always been used to market these products.
Likewise, as more and more new investigations of the vaccine program emerged around the globe, Stanley Plotkin, who many consider to be the father of vaccinology, made a startling admission:
Postauthorization studies are needed to fully characterize the safety profile of a new vaccine, since prelicensure clinical trials have limited sample sizes, follow up durations, and population heterogeneity.
Which dispels another one of the common lies we hear—that vaccines are the most rigorously tested products on the market (something I would argue is irreconcilable).
Note: in the first half of this series, I discussed a recurring issue with vaccines—their manufacturing process inevitably leading to hot (toxic) lots being produced and injuring many as nothing is done to catch the (“safe and effective”) lots before they hit the market or withdraw them once the injuries emerge. In that article, I showed how this tragedy has repeated itself again and again for over a century and since the medical profession is largely unaware of it, during the COVID-19 vaccine campaign again and again we watched large groups of people be injured by these lots but have few if any doctors sound the alarm about those hot lots.
The Risks and Benefits of Each Vaccine
While I am not the biggest fan of vaccination, I also believe that it is a mistake to be a zealot on either side of the issue i.e., “all vaccines are safe and effective” or “all vaccines are poison you should never touch”. Rather, I believe that the risks and benefits of each one must be understood as some are much more dangerous or unjustifiable than others.
Unfortunately, due to the success of the “safe and effective” mantra, whenever a legitimate criticism is brought up against a specific vaccine, it inevitably is greeted with the blanket faith that applies to all vaccines assuming they are the same (e.g., when many people complained about what the spike protein gene therapies were doing to them rather than being listened to, they simply were dismissed as “antivaxxers”).
Because the safety and efficacy of vaccines vary greatly, and parents frequently contact me asking which vaccines they should give their children, I wrote a popular article (e.g., it’s gotten a few million views on Twitter) attempting to address this question.
Unfortunately, that article had to be on the long end, the question itself is quite complicated as a lot goes into calculating the risks and benefits of each vaccine. Much of this comes from the fact you are giving yourself a known risk (as no vaccine is 100%) in return for a possible benefit (preventing you from possibly suffering a disastrous but unlikely complication of a disease you might never catch) and the fact that most of the data which would be necessary to accurately make that calculation being unavailable to the public.
Nonetheless, even with a significant amount of missing information, it is still often possible to determine if the risks outweigh the benefits.
For example, it’s well-known that children have close to a 0% chance of dying from COVID-19 (with the extremely rare cases that do happen typically occurring in severely immunocompromised children) and that they have a very real risk of suffering a significant, severe or fatal complication from the vaccine.
Likewise, the risk a girl has of developing cervical cancer from an untreated HPV infection is fairly low to begin with (especially since the existing screening methods for preventing cervical cancer have fairly effective at eliminating it) and it is actually fairly unclear to what degree the HPV vaccine prevents cervical cancer.
If we take America for instance, each year, 0.0024% of women are killed by cervical cancer (a rate which was steadily dropping prior to the HPV vaccine hitting the market), and in the first 12 years Gardasil was on the market, it dropped to 0.0022%, meaning at best, it saved 0.0002% of women. Furthermore, the rate at which the cervical cancer rates were dropping significantly slowed after the HPV vaccine hit the market (suggesting it caused rather than prevented cervical cancer—especially given that the trials for the vaccine found those with a pre-existing infection at the time of vaccination were much more likely to get cervical cancer).
Conversely, the Gardasil HPV vaccine trials showed that 0.133% of the adolescent girls who received the vaccine died (compared to an expected death rate of 0.0437%), indicating that Gardasil killed 0.089% of recipients in return for potentially saving around 0.0002% of them, and hence in the best case scenario killed over 400 times as many people as it saved. Worse still, somewhere between 2.3% to 49% of the individuals who received Gardasil developed a new autoimmune condition, many of which were extremely debilitating (with the exact amount being unknown since Gardasil’s manufacturer deliberately hid it). Worse still, beyond Gardasil being worse than nothing if you already had an existing HPV infection, its “protection” is only temporary and hence requires you to expose yourself to the same risk each time you want to be shielded from catching an HPV infection which could give way to cancer.
Thus, I believe it is fair to argue that the existing evidence and logic should make it very clear that these two vaccines should never be given to our children. Unfortunately, one of the most common tricks in marketing is to narrow our focus to a very specific point and become unable to see the rest of the picture. For example, the COVID vaccines were marketed on the basis of the disastrous COVID complications which sometimes befall children and their risk of passing the virus to their relatives, while the HPV vaccine was marketed on the basis of creating hysteria about cervical cancer and using all the fears surrounding cancer to paint that vaccine a miraculous cure for the condition we desperately needed.

Note: Merck’s One Less Campaign won awards for its effectiness.
As a result, despite the FDA and CDC being deluged with complaints about injuries from each of these vaccines, they kept on insisting the benefits greatly outweighed the risks of the vaccines, did everything they could to bury the injuries from those vaccines, and by and large (at least until recently) got the entire public to adopt the “safe and effective” narrative.
While the other vaccines on the current CDC childhood vaccine schedule aren’t quite as egregious as the COVID-19 and HPV vaccines, there are still many cases where the risks clearly outweigh their benefits (e.g., in the previous article I discussed some of the clear risks with the polio vaccine—something we still give all our children despite polio not existing within America). Conversely, others are much more ambiguous, as some degree of benefit exists from the vaccine which has to be counterbalanced against its harms (all of which is discussed in the longer article which explores the risks and benefits of each of those vaccines).
Note: while specific issues can be traced to specific vaccines, the broader problem is the chronic immune dysfunction most vaccines create (especially as more of them are given) that leads to a myriad of chronic and debilitating autoimmune or neurologic disorders that are now far more frequent than the diseases we vaccinate against. For instance, while research in this area is generally prohibited all the existing studies that have been conducted have found that vaccination vastly increases the risk of common chronic childhood illnesses (e.g., asthma or ADHD) by 2 to 10 times—and sometimes more, and there is also evidence suggesting it affects even more people with a variety of subtle illnesses that are difficult to diagnose (all of which is described in detail here). As a result, I believe if vaccines are to be taken, a good justification is needed for each one under consideration, and only the ones with the best reward to risk ratio should be taken.
Types of Vaccines
One consequence of decades of marketing around vaccines has been people assuming they have comparable risks and benefits. Another has been that they all work in a similar way (hence why experimental gene therapies could be pitched as “just another vaccine”). In reality, there are many important differences between their designs, which makes it possible to predict much of what a vaccine will actually do once it hits the marketplace.
For example, most vaccines are injected into the body (as this makes them much more feasible to deploy). However, most infections (besides exceptions like those from a mosquito or a tick) aren’t. In turn, the body has a series of immunological responses to each stage of an infection, and a very different response is provoked by vaccination that would result from the body simply being exposed to an infectious organism that passed into the respiratory tract.
Because of this, injected vaccines rarely prevent one from getting infected and colonized by a respiratory virus—rather, if they work, they typically just reduce the symptoms of a later infection by mitigating what it can do within the body. This is a very important point because whenever it becomes hard to make the case that the benefits of a vaccine outweigh its risks, the standard fallback position is that the public health benefit of preventing the disease from spreading in the population outweighs the risks one personally entails from the vaccine.
To illustrate, with COVID-19, we were initially told COVID-19 was a lethal threat and that we were incredibly lucky to be one of those who was fortunate enough to get one of the extremely limited vaccines. Then once the initial enthusiasm wore out and the vaccines were everywhere, we were given prizes and gift cards to vaccinate (many of which were absurd such as CNN promoting daily free donuts and drugs, alcohol or a free brothel session being given out for vaccinating) under the justification we were doing a civil service and helping the country by ending COVID-19.

Note: many more of absurd marketing campaigns we saw for the COVID-19 vaccines are detailed here. If you know of any truly obscene ones I didn’t include, please send them to me (e.g., in a comment) so I can add them here. I believe it’s important that the madness we went through during this time is well documented so the generations that follow us can learn from it and not repeat the same mistakes.
Finally, once the bribes stopped working, harsher and harsher mandates were instituted under the justification that they would stop the spread of COVID-19 and it was morally repugnant to put your fellow countrymen at risk of dying.
However, if you take a step back, it should be clear all of that was based on a few false premises.
One of them was that the vaccines would prevent transmission of COVID-19, something injectable vaccines rarely do (rather if anything, they increase transmission by reducing symptoms and hence making individuals silent spreaders of the disease). Furthermore, when the clinical trials for the vaccines were being conducted, outside experts pointed out they were not designed to assess if the vaccines would reduce transmission, and likewise when the pivotal vaccine clinical trials were published, they did not state that the vaccines reduced transmission (rather they simply studied if symptoms of a COVID-19 infection were reduced). Nonetheless, our public health authorities continually insisted they did (as they pushed for more mandates)—even as more and more evidence accumulated showing they did not.
Note: what I found remarkable about this was not that our public health authorities lied, but rather that few if any doctors I spoke to recognized this lie—including holistically minded ones to whom I clearly explained the science (rather they kept saying “if it reduces your chance of getting COVID-19, that means it reduces your chance of transmitting COVID-19”—which likewise demonstrated that they didn’t understand what was actually tested for). This I would argue is similar to how many doctors insisted on wearing masks even after it was shown COVID-19 had an aerosol rather than droplet spread which hence made masking completely pointless (as virus aerosols easily pass through the gaps in masks), and still continued to wear them after large studies showed masking offered no benefit.
In short, I would argue those events highlight the importance of understanding the different types of vaccines. Had this been common knowledge, the public would have refused to follow any mandate of the COVID-19 vaccine that was not designed to create immunity within the nasal mucosa (which remarkably prominent voices in the industry like Bill Gates have now started advocating for since the injected ones failed to prevent transmission).
Note: this article discusses why vaccines consistently fail to prevent disease transmission and the types of vaccines that create mucosal (IgA) immunity (e.g., intranasal sprays, and certain live virus preparations).
How Vaccines Work
The immune system has a variety of functions (e.g., it repairs tissues after injuries), and of these, it is most well known for its ability to eliminate or neutralize things that should not be in the body (e.g., toxins, infections, or cancers). In turn, since it performs such a vital function, a significant portion of the body’s resources are dedicated to supporting it (e.g., the total weight of all the immune cells traveling throughout the body is roughly equivalent to 2.6 pounds, which is comparative to the weight of the liver).
For the immune system to perform this job correctly, it has to do three things:
•Be able to effectively eliminate its target.
•Be able to respond faster than the threat can proliferate within the body.
•Cause minimal collateral damage to cells and tissue of the body.
Note: in many cases (e.g., due to vaccines) the immune system partially or fully loses the ability to do this and instead develops an “off-target” immunity which fails to eliminate the threats we face and instead attacks the body (causing one of many autoimmune disorders).
In order to meet the balancing act of only responding to the correct threats, the immune system has an adaptive capacity which allows it to rapidly scale up its ability to respond to a critical invader.
This process essentially works as follows (although in reality it’s much more complicated):
•The body continually produces immune cells with slightly different protein sequences, which, due to a random rearrangement process and a massive number of cells being present, collectively ultimately end up containing enough protein sequences for them to match any threat the body will encounter.
•When one of those cells contacts a threat inside the body that it “matches” the protein (antigen) sequence of, it begins reproducing so a large number of cells exist which can eliminate that invader.
• Once the threat is eliminated, some of the cells remain so that if the threat returns, the body can activate a much faster response to it.
Note: a gland in the body also eliminates immune cells that match normal tissues, preventing the development of a destructive autoimmune response.
One of the big problems with this process is that the immune response takes time to develop, so in some cases, by the time that’s happened, the invading organism will have already had time to multiply enough within the body to cause significant issues (and in some cases death). Fortunately, as more of the organism is present, there are more opportunities for the matching immune cell to contact it and start developing an immunity to it, so typically, the immune system heads off infections before they’ve had too much time to progress.
The theory behind vaccination hence is that if you can expose the body to the antigen sequence of something you want it to develop immunity to (without a dangerous replicating organism being present), it makes it possible to develop an immune response that can then rapidly kick in once the actual invading organism is present.
To accomplish this, vaccines put a predesigned antigen into the body (e.g., the COVID vaccines inject the spike protein into the body under the theory that COVID-19 requires the spike protein to enter the cells and reproduce, so if the immune system can neutralize the spike protein, COVID-19 infections can be quickly halted by the immune system).
Unfortunately, in real life, this is often quite challenging to do. That is because:
•Producing the target antigen sequences can be quite costly.
•The body often does not have a sufficient response to the antigen sequence.
•Since the antigen sequences are typically sourced from microorganisms, producing the vaccine requires culturing microorganisms, which in turn leads to contaminants from that culturing entering the final vaccine (e.g., in the previous article, I discussed dozens of disasters that arose over the decades from dangerous contaminants existing in the final vaccine product that was injected).
•The antigen sequence by itself is often quite toxic to the body. The best example of that is the spike protein (hence why individuals who receive vaccines which mass produce the spike protein within the body become quite ill), but as I showed in the previous article, it was also a major problem with the “dirtier” vaccines which were sourced from mass produced bacteria (e.g., pertussis or anthrax) which were killed and then turned into injectable antigens. Likewise, if a toxin (e.g., from tetanus or diphtheria) added to the body with a vaccine is not sufficiently deactivated, that toxin can injure or kill the recipient (which as I showed in the previous article has happened numerous times in the past).
•The chemicals needed to inactive the toxic components of the vaccine (e.g., a virus or toxin) are often also toxic to the body.
Antigen Production
Over the years, a variety of increasingly genetically engineered approaches have been created to create the needed antigens. The six main ones are:
1. Growing large amounts of the infectious organism, doing something to “kill” it, and then attempting to filter away everything besides the desired antigens of the organism or its neutralized toxin (which is how most vaccines for bacterial infections are produced).
2. Culturing a virus in a medium (e.g., annual flu vaccines are grown in eggs while the polio vaccine is grown in monkey kidney cells) and then inactivating the antigen containing virus by exposing it to a chemical. In most cases, this takes a while, which helps to explain why the annual flu vaccine is almost always for a different strain than the one that actually emerges (as they have to start producing the vaccine long before the dominant flu strain is known and hence must rely on their best guess to determine what the strain is).
3. Genetically modifying an organism to produce the target antigen sequence, then killing the organism and extracting the antigen sequence. For example, both the HPV vaccineand the hepatitis B vaccine antigens are made from genetically modified baker yeasts. Newer approaches, such as growing the antigen from plants or insect cells (e.g., Novavax was made from moth cells), are also now beginning to enter use.
4. Modifying an organism so that it remains capable of reproducing within the body, but is less likely to cause a severe illness. Some of the common live attenuated vaccines include the measles mumps and rubella vaccine, certain flu vaccines (e.g., the nasal ones), the chickenpox and shingles vaccines, and the live oral polio one (which is not given in the United States). A few bacterial ones also exist (e.g., for tuberculosis or typhoid fever).
5. Modifying a relatively harmless virus to also carry a target antigen sequence (e.g., the spike protein) and then having that virus mass reproduce within the body. The most well known examples of this were AstraZeneca, J&J’s, Russia’s (Sputnik), and China’s Convidecia COVID-19 vaccines. Previously it has also been done for Ebola.
6. Transfecting human cells with mRNA which causes them to produce the target vaccine antigen.
The essential challenge all of these approaches face is that enough of the costly antigen needs to be produced for the immune system to develop a durable immune response to it. The original solution the vaccination field developed was to mix the antigen with a much cheaper additive which enhanced the immune response to the antigen, thereby making less of the costly antigen needed. Unfortunately, those adjuvants tended to be toxic (e.g., I believe one of the primary issues with most vaccines is the tendency of their aluminum adjuvants to cause microstrokes in the body and create autoimmune disorders).
Note: a textbook has been written on how aluminum causes autoimmune disorders, while other papers have shown how the immune system shuttles it into the brain after vaccination. While I cannot prove this, I have long believed the reason why aluminum functions as such an effective stimulus for the immune system is due to its strong ability to destroy the physiologic zeta potential, as this is something that would also occur in most infections and hence serve as a nonspecific signal to the immune system and something that could be detected from far away (due to how it distorts the water of the body).
As time has passed, the vaccine field has moved towards using genetic engineering to efficiently produce the target antigen, either outside the body (e.g., in yeast cells) or within the body through some type of self replicating technology (e.g., the viral vectors or mRNA technology). As these approaches are highly unnatural, we are in turn continually discovering new consequences of them.
For example, the mRNA technology overproduces spike protein within cells, leading to it being forced out onto the surface of the cells, at which point the immune system not only recognizes it but the entire cell as a threat, which in turn helps to explain why profound in autopsies of those who died from the vaccines experienced things such as tissue destruction due to immune cell infiltration that examiners described as:
This combination of multifocal, T-lymphocyte-dominated pathology that clearly reflects the process of immunological self-attack is without precedent.
However, while many issues exist with each of these approaches for designing vaccines, in my opinion, the primary issue is that all of those methods produce an excessive immune response to a single antigen, rather than a moderate immune response to a wide variety of antigens (which is what happens during a natural infection).
Note: live viral vaccines don’t have this issue (as they contain the wide range of antigens normally found on a virus). Unfortunately, since they are live, they also will reproduce within the body, and hence some hesitancy exists towards their use (e.g., immunocompromised individuals are advised against getting them and sometimes nonetheless become ill from shedding in the community of those live viruses).
Single Antigen Vaccines
Typically, the immune system does not produce an excessive immune response to a single antigen. However, if enough of it is put into the body or the body is exposed to adjuvants which provoke it into responding, it will. In turn, there are a few key issues with doing this:
1. The process of provoking the immune system to develop an excessive immune response will also frequently cause it to develop an immune response to other antigens in the vicinity. If those antigens are human tissue, this leads to autoimmunity (a common side effect of vaccines)—especially if the vaccine antigen overlaps with human tissue.
For example, the hepatitis B vaccine has a significant overlap with myelin (which coats your nerves and thereby allows the nerves to function). Because of this, debilitating demyelinating disorders (e.g., multiple sclerosis) have been associated with hepatitis B vaccination, and one study showed approximately half of its recipients also developed immune reactivity to myelin (which in the majority of cases persisted for over 6 months).
Likewise, one study showed that mice developed allergies to pollens that were in the air at the time of their vaccination.
2. The simplest type of mutation which occurs in nature is the changing of a protein sequence. Since protein sequences have to match for an immune response to occur, creating a strong immune response to a single antigen immediately creates a selective pressure that causes the pathogen to evolve into something which no longer has the matching antigen. This for example is why the COVID vaccines being released onto the market( which primed the body to respond to a very specific spike protein) rapidly led to variants emerging which had different spike proteins the vaccine no longer worked on.
To a large extent, this process can be avoided if the vaccine targets an essential antigen for the organism that cannot mutate without losing its function (hence causing the mutation to kill the organism) or multiple antigen sequences are present on the vaccine so that even if the resistance to a single antigen spontaneously emerges, the immune system can still neutralize the pathogen through its other antigens (and hence prevent that resistance from entering the microbial population). However, as mentioned before, most vaccines (except say the live attenuated ones) do not have multiple antigens.
Note: in certain cases, selective pressure does not exist. For example, since the tetanus bacteria lives throughout the environment in the soil and does not depend on human beings to reproduce, it is exceedingly unlikely that vaccinating humans will cause its toxin to become resistant to a vaccine.
3. The previous point is particularly problematic because while the immune system has an immense ability to respond to threats, its capacity is still limited. Because of this, if its focus is diverted to responding to a very specific antigen (e.g., due to a strong adjuvant triggering it or the antigen continually being produced within the body after a mRNA vaccine), it loses the ability to address other threats (e.g., new variants). Many examples of this exist. One of the best known examples occurred when one of the WHO’s top vaccine researchers discovered that giving the DPT vaccine in a region of Africa where people frequently died of infectious diseases caused children to be 5 times as likely to die (boys were 3.93 times and girls were 9.98 times more likely to die).
Likewise, many studies (detailed here) have shown that getting flu shots increases one’s risk of getting the flu if the shot does not match the annual strain (which is what almost always happens). For example:
A 2009 study found that vaccinating mice for influenza removed their ability to develop resistance to pandemic influenza following previous exposure to normal influenza. Compared to unvaccinated mice, vaccinated mice continued to lose body weight after a pandemic influenza infection and had 100-fold higher lung virus titers on day 7 [this increases transmission] post-infection and more severe histopathological changes.
•A 2010 review of four studies found that recipients of a seasonal influenza vaccine had a significantly increased risk (ranging from a 40% to 150% increase) of subsequently developing severe pandemic influenza (which unlike normal influenza could hospitalize you).
•A 2010 study of the severe pandemic influenza found that active duty members of the military were more likely to have received influenza vaccination than were those without H1N1 virus infection.
•This 2012 study conducted between 1999-2007 of 261 children 6 months to 18 years old who developed laboratory-confirmed influenza found that infected children were 267% more likely to be hospitalized if they had previously received an influenza vaccine.
•A 2012 study randomized 69 children to receive an inactive influenza vaccination, and 46 to receive a placebo. Of those vaccinated, 29.0% developed an infection with a non-influenza upper respiratory virus, whereas 3.4% of those who were not vaccinated developed an upper respiratory infection from a non-influenza virus.
•A 2013 study found receiving an influenza vaccination two years in a row increased rather than decreased the likelihood of developing influenza by 45% (ranging from 6% to 148% depending on one’s age).
Note: there is very little evidence influenza vaccination provides any benefit. For example, this 2013 Cochrane review (which represents the most objective and comprehensive evaluation of the existing evidence) found there is no benefit in giving them to children, this 2012 review found there was no benefit to patients if healthcare workers received them (nonetheless they are still mandated for most healthcare workers) and this 2006 study found our national vaccine program had provided no reduction in influenza for the United States.
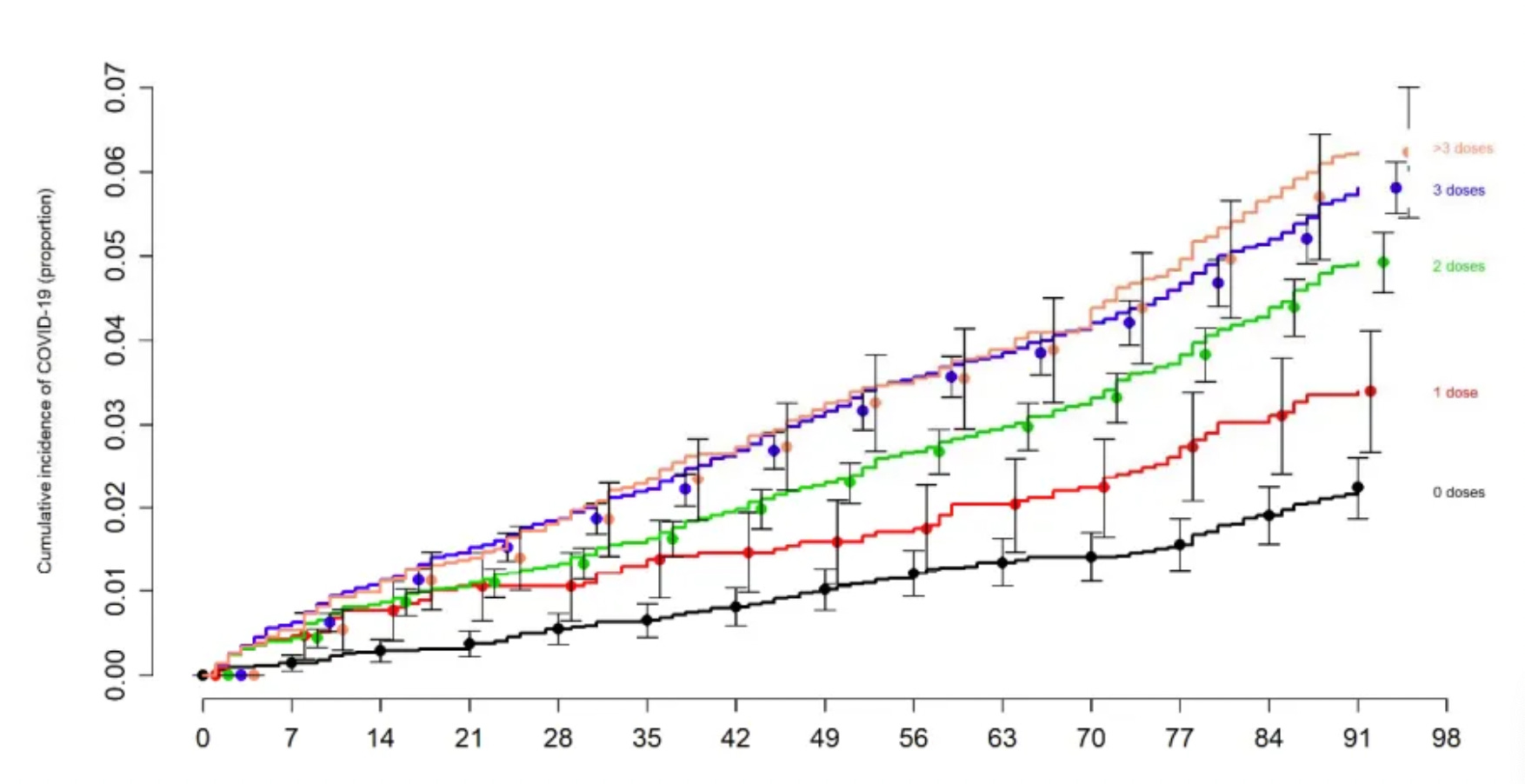
Finally, we also witnessed throughout COVID-19, as we’ve all seen that those who were repeatedly vaccinated kept on getting COVID, whereas those who got the infection naturally developed a durable immunity. This was best shown by the Cleveland Clinic’s study of 51011 people, which found the more (single antigen) vaccines one got, the more likely they were to get COVID-19.
4. An introductory principle in immunology is that there is a constant balance between the Th1 (cell mediated or cytotoxic) immune response and the Th2 (humoral or antibody) immune response as the Th1 response releases IFN-γ which effectively suppresses the Th2 response, and the Th2 response releases IL-4 and IL-13, both of which effectively suppress the Th1 response. The Th1 response tends to be excellent at dealing with intercellular pathogens and cancers, while the Th2 response tends to be excellent at dealing with pathogenic substances such as toxoids, parasites and encapsulated bacteria that are outside cells or on their surfaces. The balance between Th1 and Th2 is frequently discussed within the hygiene hypothesis, which posits many of our chronic diseases arise from an imbalance between these two systems due to modern sterile living conditions.
Classical vaccinations (those with a small number of antigens and an adjuvant such as aluminum) tend to excessively increase the Th2 response (e.g., see this study on the DPT vaccine). Likewise, there are a variety of effective conventional and alternative medical therapies that elevate the Th1 response and suppress the Th2 response which are often used to treat complications from vaccinations, cancers, or viral infections.
Because of this, you typically observe the best results for single antigen vaccines which are directed against toxoids or encapsulated bacteria. However, at the same time, these vaccines often stop working because they place selective pressure on the organism to evolve resistance. This is best demonstrated with the pneumococcal vaccine, which as the years have gone by, has had to have more and more antigens added to it so that the existing strains are still covered by the vaccine.
Note: live viral vaccines tend to give a more natural and functional immune response with both a Th1 and Th2 response (e.g., see this study on the MMR vaccine).
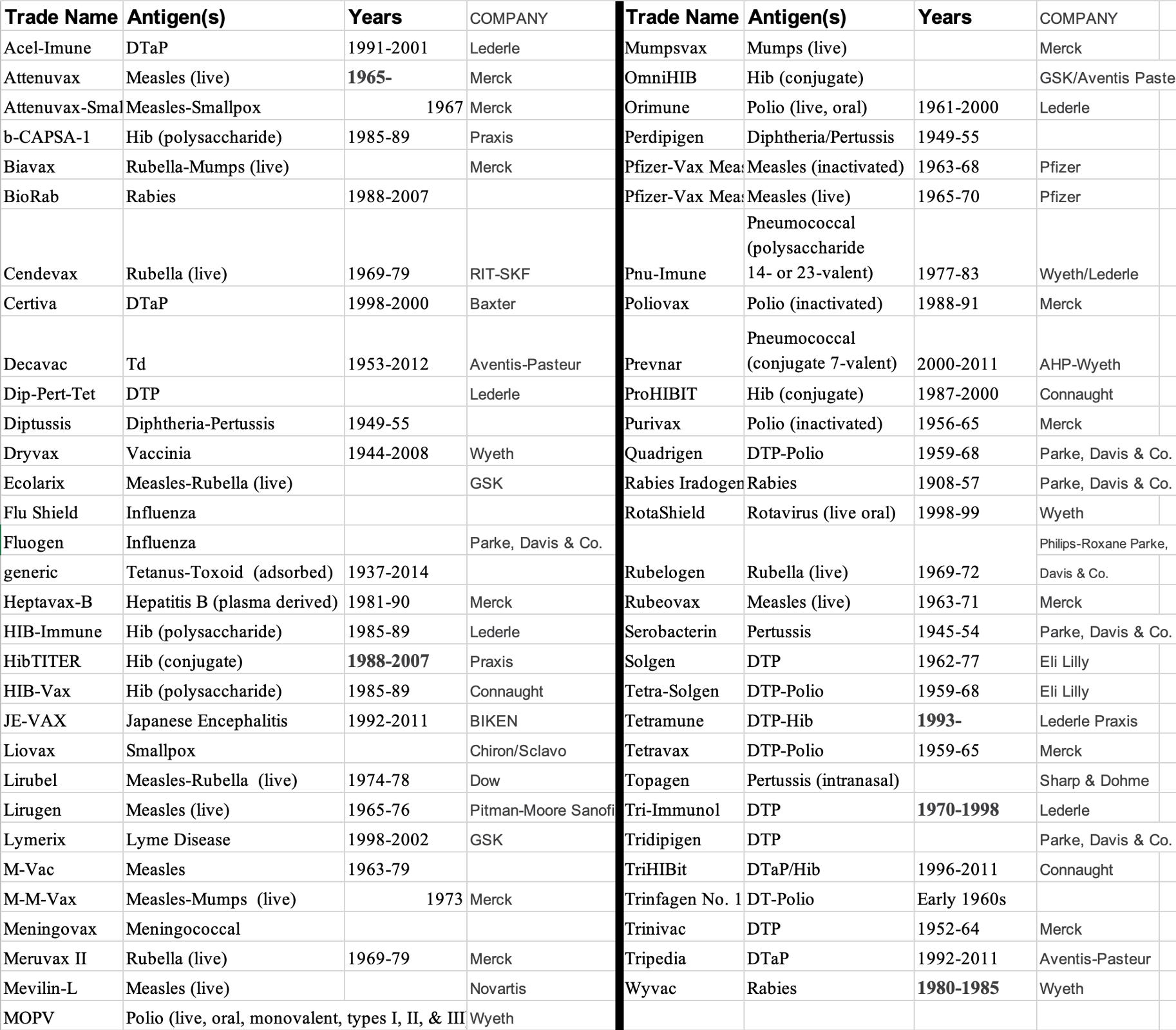
Withdrawn Vaccines
A key fact many people do not appreciate about vaccines is that despite the vaccines being “safe and effective” many have been withdrawn from the market, and it is likely many more (e.g., some of the COVID vaccines) will be in the future. For example, this is one list of withdrawn vaccines that was compiled:
Justifiable Vaccines
As I’ve tried to show thus far, there are serious issues with many of the existing approaches to vaccination that have largely been buried and forgotten because too many have been led to believe “all vaccines are safe and effective.” Now, however, I’d like to look at it from the opposite end of the spectrum. Which vaccines do the best justifications exist for?
Natural Immunity
In most cases, the most effective vaccine is one which develops from natural immunity. Because of this, in most cases, my preferred approach to “vaccination” is to try to have the tools on hand to help someone with the infections they have and do everything I can to help nurture both a recovery from the illness and a robust immune response to it.
For this reason, I try to encourage patients not to be deficient in the basic nutrients that facilitate immunity (e.g., zinc, vitamin C, vitamin D, and sunlight), to know the simplest ways to treat common infections (e.g., I listed the most easily available approaches for treating COVID-19 here—many of which also work for other illnesses like the flu), and when a patient gets ill, I try to encourage a robust immune response (e.g., I typically encourage patients to heat their body rather than taking fever suppressants, and if I frequently provide ultraviolet blood irradiation for the more severe illnesses as it typically fully resolves them).
Overall Mortality
The major issue with this approach however is that in many unfortunate cases, individuals simply do not have access to the medical care they need when they get ill, and likewise, it’s unlikely our medical system will ever adopt many of the measures I believe could prevent severe illnesses. In turn, the strongest argument for vaccines is if they can accomplish their promise to guarantee immunity for a dangerous illness, as it is far more feasible to mass distribute an effective vaccine than it is to ensure everyone will always have access to the care they need for the illness.
However, as we try to identify those vaccines, we touch on one of the largest issues with modern research—it’s so easy to doctor research and rearrange the existing data to support a sponsor’s narrative that it’s actually quite difficult to know for sure if a therapy is or is not beneficial. In turn, as I’ve looked at the existing vaccines that are recommended by the CDC, I’ve only been able to identify one where it seems that a strong argument can be made for the vaccine, and a few where I believe a strong argument existed in the past but now is no longer applicable (e.g., because the infectious agent evolved a resistance to the vaccine antigen or because the infectious agent, while dangerous in the past, no longer exists now).
Note: the risks and benefits of each childhood vaccine are discussed in further detail here.
Typically, the most effective way to cut through all the deception in modern research is to see how many people who receive an intervention die (known as “overall mortality) and compare that to the death rate of those who never received the treatment. In the case of vaccines, this metric is rarely reported (as a net mortality benefit rarely exists for the vaccines we give our children), and in many cases, the exact opposite is seen instead (e.g., as mentioned before, Gardasil increased overall mortality, and likewise, at 6 months of follow up, Pfizer’s data [in table S4] showed that while the vaccine “prevented COVID” those who received it were more likely to die than those who did not).
From looking into this question extensively, I have only ever been able to find two vaccines that were demonstrated to decrease overall mortality when given en masse—the MMR vaccine and the BCG (tuberculosis) vaccine. However, there was a caveat; this benefit was only seen in areas where children frequently died from infectious diseases, and the reduction in death (which ranged from 38-86%) was primarily due to the myriad of other diseases (which the vaccine did not target) becoming less lethal. Conversely, as mentioned before, immunosuppressive single antigen vaccines (e.g., DTwP) had a far larger increase in a child’s risk of dying.
The MMR and BCG data in turn highlight an important point—the immune system works better if it is trained to eliminate natural infections, and in many cases live viral vaccines are the best way to do that. For example, there is a large body of evidence which shows a failure to get many of the common childhood illnesses makes individuals be much more likely to contract severe illnesses later in life. To illustrate:
•Not having a chickenpox infection increases your risk of brain cancer later in life (e.g., see this study, this study, this study, and this study).
•Not having a mumps infection increases your risk of ovarian cancer, one of the most deadly cancers for women (see this study, this study, this study).
Note: this preventative effect was also found for measles, rubella, and chickenpox infections.
•Previous infections of influenza, measles, mumps, or chickenpox were found to decrease one’s risk of malignant melanoma.
Note: another study found similar results.
Therapeutic Vaccines
In certain cases, vaccines are given to patients not to prevent them from getting a disease but rather to mobilize the body to expel a disease that is already present. For example, the BCG vaccine has been observed to provoke an immune response that treats bladder cancer, and as a result, it is a standard therapy for bladder cancer. Similarly, many patients with chronic recurring shingles found the same when taking the shingles vaccine.
In my eyes, these scenarios make it much easier to assess the actual benefit of a vaccine, as you can compare the vaccine’s known risks to a clear benefit rather than a speculative one far into the future (e.g., the HPV vaccine preventing a lethal case of cervical cancer). In turn, there are a few instances where a live vaccine can be used therapeutically (e.g., the BCG vaccine shingles vaccine) and that calculation can be made. Of these, I believe the strongest argument exists for the rabies vaccine if it’s needed as a therapeutic intervention after a rabid animal bite, as while the rabies vaccine is harmful, a rabies infection is typically fatal, but this can be prevented if a vaccine is given after a bite (as the rabies infection progresses slower than the immunity the vaccine creates).
Note: conversely, the two arguments I know against the above points are that individuals sometimes unnecessarily receive the vaccine (e.g., prior to it being discovered the animal did not have rabies), some of whom then are injured without any benefit existing from vaccinating, and the fact that to some extent, rabies can be treated with ultraviolet blood irradiation (although I only know of a few cases of this, so I simply isn’t enough data to justify using it in place of an otherwise necessary treatment).
Additionally, more and more immunotherapies are being created which essentially use a vaccination approach to stimulate the immune system to eliminate the tumors existing within it. Some of these work by provoking the immune system to attack a tumor (e.g., the BCG vaccine and a genetically modified adenovirus do this for bladder cancer, while a genetically modified herpes virus does this for melanoma), while others do this by taking immune cells out of the body, priming them to be responsive to the cancer and then putting them back into the body (e.g., one of these exists for prostate cancer).
Ideal Vaccines
Ideally, a vaccine should be safe enough that it is highly unlikely to injure its recipients, and simultaneously able to provide a concrete benefit that justifies the cost of its deployment. In this article, I’ve tried to show how many obstacles exist to a vaccine being able to do this. While many of these can potentially be overcome with improved technology (e.g., some of the newer methods of commercially producing large amounts of a target antigen through creating applications of genetic engineering have the potential to make the vaccine production process much cleaner and less likely to come to market with numerous “hot lots”).
Nonetheless, I also believe that under the current paradigm (introducing foreign proteins and organisms into the bloodstream), it is unlikely if not impossible to produce vaccines that are free of side effects.
From having looked into this question extensively (I often like to deeply explore both sides of an argument—especially ones where I hold strong preconceived beliefs), I have ever only been able to identify two vaccine technologies that clearly and unambiguously benefit their recipients.
Sadly, very few people know of either of these approaches, which is unfortunate as one offers a way to economically and safely address a variety of otherwise devastating infectious illnesses (e.g., by preventing them in a safe manner that does not require immunizations), while the other is sometimes utilized within the integrative medical field to cure a variety of debilitating and chronic illnesses (e.g., chronic fatigue, rheumatoid arthritis and Lyme disease). As each of them relates to a highly controversial therapy (that I frequently am asked questions about here), I believe that in part explains why there is so little knowledge of these approaches, so in the final part of this article, I will discuss each of them.




No comments:
Post a Comment