
Is it possible to avoid heart damage from the COVID vaccine? Or do all COVID-vaccinated people have some myocarditis?
The following peer-reviewed paper may be found at Primary Doctor Medical Journal.
Abstract
This paper addresses the question of prevalence of COVID vaccine-associated myocarditis, as well as known mechanisms of spike protein-induced myocarditis, considering the epidemiological consequences of mass vaccination with spike protein-generating COVID vaccines, such as are being deployed throughout the world at present. The cardiac impacts of spike protein distribution have risen to particular concern, due to the recent extraordinary increase in new cases of myocarditis and pericarditis, including among populations that typically have vanishingly rare incidence of this disease, especially young men, with particularly anomalous occurrence in young male athletes.
Introduction
The US Centers for Disease Control and Prevention (CDC) finds increased reported cases of myocarditis and pericarditis following mRNA COVID-19 vaccination, most notably in adolescents and young adults, [1] including in the absence of COVID-19 infection. [2] Myocarditis was only rarely found post-vaccination prior to the COVID mRNA vaccines, and then mostly associated with the smallpox vaccine. [3] Typically and historically, myocarditis patients are older with high prevalence of diabetes, hypertension, atrial fibrillation, coronary artery disease and heart failure. [4] Myocarditis is an extremely concerning condition. At five years post-diagnosis, myocardial injury, which is a clinically indistinguishable condition from myocarditis, and often discussed interchangeably and synonymously, is correlated with a 72.4% mortality rate, and is therefore correlated with higher mortality than even Type 1 myocardial infarction (rupture of coronary artery plaque with thrombus) or Type 2 myocardial infarction (vasospasm generally), which have 36.7% and 62.5% five-year mortality rates respectively. [5] So myocarditis is likely even more concerning than myocardial infarction. This may be due to the generalized cytotoxic injury, due to external cause, throughout the heart in the myocarditis event, compared to the localized watershed damage affecting a portion of the heart, which is associated with myocardial infarction.
Heart function is mostly regulated by cardiomyocytes and vascular endothelial cells. Cardiomyocytes have no potential for self-renewal, as they are terminally differentiated cells. When they die, they necrose and are replaced by proliferating fibroblasts, which form fibrotic tissue. This tissue reduces systolic function, and is associated with a poor prognosis. [6]
Due to the generally much higher activity level of a young athlete than of the historical prototype myocarditis patient, are we simply noticing greater contrast in activity level before and after the COVID vaccines in the former, and missing this contrast, and hence the myocarditis diagnosis, in more sedentary individuals? This paper will examine the possible mechanisms of the mRNA COVID vaccine association with myocarditis, in order to assess how common this association might be.
When asked in June 2021 about the risk of myocarditis following the COVID vaccines, Dr. Roger Hodkinson, pathologist, replied:
“Myocarditis is never mild, particularly in young healthy males. It’s an inflammation of the heart muscle, the pump of the body. And we don’t know what percent of the heart muscle cells would have died in any one attack of myocarditis. The big thing about heart muscle, heart muscle fibers, is that they do not regenerate, . . . so you’re stuck with an unknown percentage of your heart muscle cells having died. We can’t estimate the number, and therefore the long-term results are utterly unpredictable. We do know . . . that myocarditis can present decades later, with premature onset of heart failure that would otherwise not have been expected. So it’s a terrible worry for these people to know what’s going to happen to them in the future. . . . It’s not trivial.”
In diagnosing myocarditis, cardiac magnetic resonance studies (CMR) have shown specific sites of inflammation or fibrosis, and help to evaluate functional impairment of heart muscle. Myocardial edema and late gadolinium enhancement are seen on CMR in cases of myocarditis. In all cases reporting chest pain post-COVID vaccine in one study these abnormal findings were present on CMR in each subject. Past or current COVID-19 disease had been excluded in all subjects. [7] However, the more widely accepted criterion of myocardial injury is a threshold of serum troponin levels at or above 99th percentile of upper reference range. [8] Elevated troponin is considered to be both sensitive and specific for myocardial damage. Troponin is a protein normally confined to the cytosol of cardiomyocytes, as well as other muscle cells, and is not normally found in the blood; however, it is released in the circulation when heart muscles become damaged.
At the time of this writing, in the current post-peak-COVID era, it has been 15 months since peak COVID mortality in the US and the world, which occurred in mid-April 2020, as shown by CDC data. [9] Now, a year later, COVID vaccines have been aggressively introduced in most countries, and Our World In Data, which is funded by the Bill and Melinda Gates Foundation, estimates that 2.5 billion people or one quarter of the earth’s population, have already taken one of the new COVID vaccines, although they have only been available for about six months. [10] As morbidity and mortality from SARS-CoV-2 and COVID-19 and its variants have diminished, and the world’s death rate per 1000 people is still at a relative low in 2020 and 2021 compared to the last seven decades, without evidence of any recent pandemic by mortality data, [11] we now can turn our attention to the health effects of the new COVID vaccines. None of the new vaccines attempts to introduce the entire coronavirus into the body, but rather a spike protein generating mechanism. Therefore, let’s focus on only the spike protein’s effects on the myocardium and its cells.
Mechanisms
Recent introduction of mRNA vaccines that program human cells’ genetic mechanisms to generate spike proteins have led to an increased interface generally between spike proteins and bodily tissues. These recently increased venues of interaction have apparently exceeded, both in human populations and in human tissues, the levels that mRNA vaccine developers had expected. For unknown reasons, mRNA vaccine researchers had expected spike proteins to remain entirely in the deltoid muscle at the vaccination site of the vaccinated person, as reported in the media, [12] and it was apparently imagined that these spike proteins could somehow evade release into the general circulation. However, it has recently been determined that the delivery of spike proteins and / or their generating mechanisms, as with all known injected substances, do indeed diffuse and travel in an organism, away from the site of injection, in accordance with well-established principles of circulation, throughout the body, including to internal organs. Organs that have been affected by this body-wide distribution have included the heart, brain, spleen and liver, with especially high concentrations found in the ovaries and the plasma. [13]
The spike protein is the part of coronaviruses in general, and SARS-CoV-2 in particular, that attaches to and interacts with human cell membranes. I examine the role of the SARS-CoV-2 spike protein on the myocardium, and mechanisms by which the cardiomyocytes and vascular endothelial cells, which predominate there, may be threatened by such exposure. It is possible that other elements of the SARS-CoV-2 virus, besides spike proteins, have deleterious effects on cells, including risk for myocarditis. [14] It has been observed also that mRNA interventions are fragile and unpredictable in their effect, [15] and have been seen to damage mitochondria by a number of known mechanisms. [16] Of patients hospitalized for COVID-19, myocarditis-pattern injury was observed in 4.5%[17] to 27% of cases. [18] Moreover, in the event of SARS-CoV-2 infection, it was found that the associated cytotoxic and pro-apoptotic effects were sufficient to abolish cardiomyocyte beating (contraction-relaxation cycles). [19] However, direct virus replication was not found on examination of the myocardium, [20] [21] and SARS-CoV-2 RNA was not found in the cardiomyocytes. [22] Therefore, it is worthwhile to examine if post-vaccine myocarditis is likely to be caused by spike proteins generated by the vaccines, and to result from either the cytokine storm or from the endothelial damage caused by spike proteins. Considering a wider set of possible causes, we know that fulminant SARS-CoV-2 infection is characterized by hypoxia, systemic inflammation, thrombosis and / or cardiomyopathy, as well as myocarditis. All of these have been observed in vitro in the presence of spike proteins, and all of these can result in higher levels of measured troponin, which in turn establishes diagnosis of myocarditis, or at least clinical awareness of signs of myocarditis. [23]
At this time, there is not any other part of the SARS-CoV-2 virus that is known to attach to human cells. The binding of the spike protein to cell membranes initiates a cascade of events that result in fusion of the viral and cellular membranes and entry of the virus into the human cytoplasm. [24] Most of this activity in most human cells seems to involve one or both of the S1 subunits of the spike protein, but for human brain endothelial cells, it seems the S2 subunit of the spike protein is involved. [25] Human host cell proteases participate in this fusion and entry. [26]
The spike proteins that are generated by the mRNA COVID vaccines are said to be identical to those attached to SARS-CoV-2. [27] The spike protein in SARS-CoV-2 is a trimeric, or three-part protein, composed of two functional S1 subunits, as well as a structural S2 subunit. Each of those three units are, incidentally, bound and inactivated by the drug ivermectin. [28] In the absence of ivermectin or hydroxychloroquine, the two drugs most thoroughly studied and most widely used in early and late cases of COVID-19, [29] the spike protein remains in a conformation that enables it to attach to the ACE2 receptor on human cells, and to enter by that portal. Conversely, either of those drugs are able to change the conformation of the spike protein in such a way that prevents entry to the human cell. [30] ACE2 receptors are found in cells throughout the human body, and have been shown to have varying effects on different organs. ACE2 receptors have been found to be highly concentrated in cardiac pericytes, [31]even more so than in the lungs. [32] But the presence of ACE2 has been observed to have a seemingly paradoxical protective effect in the cardiovascular system, such as preserving ATP production. [33] Spike proteins have been found to down-regulate ACE2. [34] Human cardiomyocytes have been observed to express the ACE2 receptor, and that is the main portal by which the spike protein of SARS-CoV-2 is observed to attach. In addition to the ACE2 receptor, the CD-147 receptor is also used by the spike protein to enter host cells. [35]
Spike protein was found to enter cardiomyocytes in vitro, and cytotoxicity was detected at 24 hours post exposure, and “profound cytopathogenic effects” were visible at 96 hours in cardiomyocytes. [36]
The spike protein alone of SARS-CoV-2 has been found to have damaging effects on endothelial function. [37] In fact, the spike protein alone was found to produce pro-apoptotic factors that were determined by researchers to be responsible for endothelial cell death. [38] Endothelial cells that were treated with the spike protein showed mitochondrial fragmentation and dysmorphic changes, as well as reduced mitochondrial respiration with redox stress, but increased glycolysis, and it was shown that the S protein alone damaged endothelial cells by this mechanism. [39] Interestingly, in those in vitro studies, cell function was found to be restored by adding N-acetyl-L-cysteine, which is a reactive oxygen species inhibitor.
The spike protein has been found, without other viral elements, to stimulate cell signaling in human cardiac pericytes that has been associated with cardiac cell dysfunction. Some of this dysfunction includes findings of increased amounts of the following pro-inflammatory cytokines (those involved in cytokine storms) in cardiac pericytes on in vitroexposure to S protein: MCP1, IL-6, IL-1B and TNF-alpha. [40] TNF-alpha is specifically associated with heart failure and myocarditis. [41]
Caspase-3 is associated with apoptosis. When coronary artery endothelial cells were exposed to spike protein, they were found to have increased Caspase 3/7 activity, which was correlated with pro-apoptotic effect. Some of the above activity was through the ACE-2 receptor, but more data showed involvement of the CD-147 receptor on those cells, [42] and we have seen above that both pathways are used by spike proteins for cell entry. The cell death experienced in myocarditis seems likely to be at least partly due to this activity.
Electrocardiogram (EKG) abnormalities have also been found following COVID vaccine administration. This includes diffuse ST elevation and an inverted T-wave in lead III, as well as sinus tachycardia. [43]
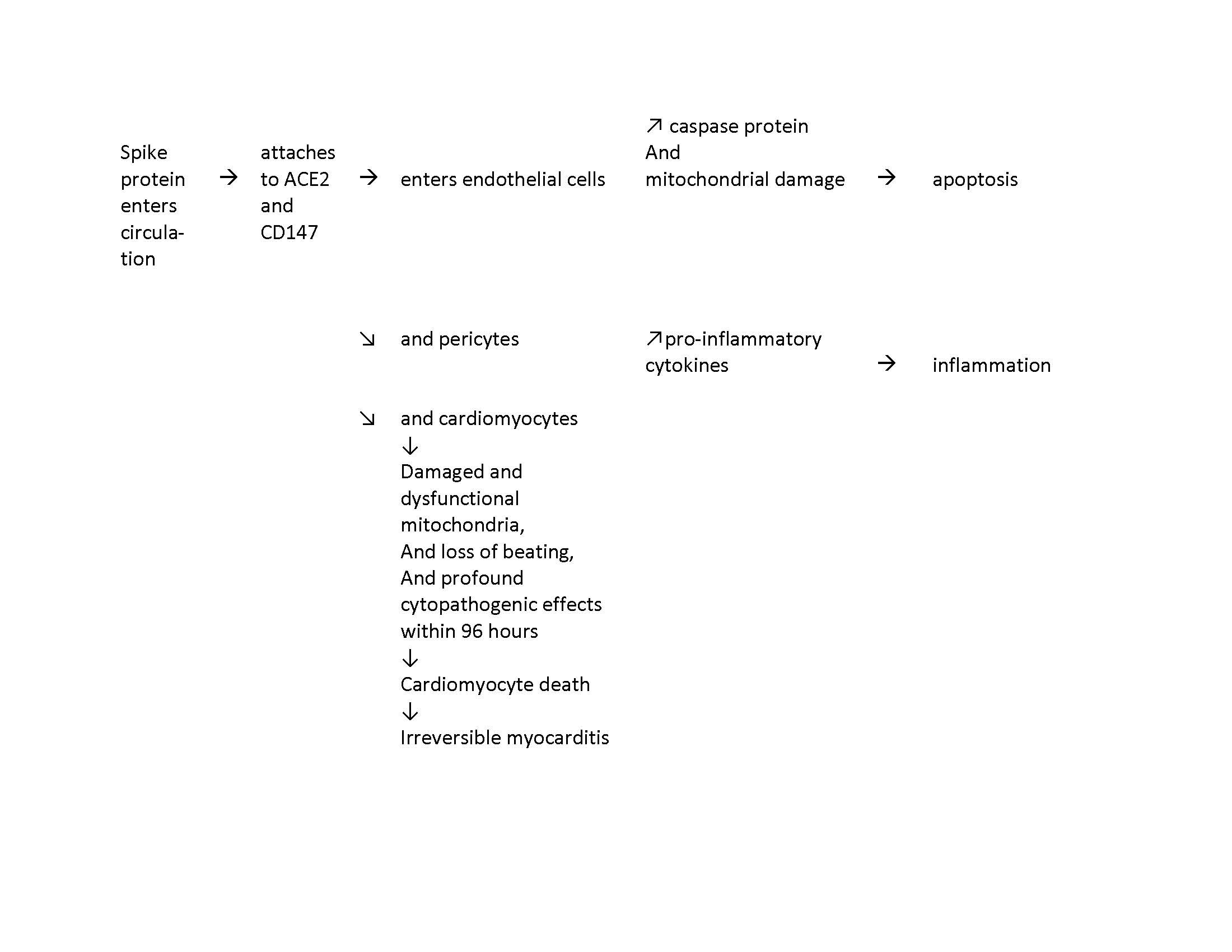
A summary of expected effects after COVID vaccination is in Figure 1.
Figure 1: Summary of cardiovascular events following COVID vaccination
Discussion
The pathways discussed herein are inevitable routes of spike protein transit in the body and in the cells. ACE2 receptors are abundant in every known cell type. When spike proteins have been introduced to the body, either through the SARS-CoV-2 virus or by means of the mRNA COVID vaccines, is there any realistic way possible to block their interaction with ACE2 receptors in any individual? In the case of acute infection with SARS-CoV-2, infected individuals have a self-limiting encounter with spike proteins, which may be thwarted by some of the therapeutics mentioned above. However, in the case of the mRNA-vaccinated, no endpoint of spike protein production is yet known. Nor is it yet known if it is safe to use any of the spike protein blocking therapeutics in vaccinated individuals.
In the absence of extraordinary and deliberate measures to block ACE2 receptors and CD147 receptors and/or Caspase 3/7 activity, is it then possible to expect that cardiac pericytes and endothelial cells could escape the pro-inflammatory and pro-apoptotic effects of the spike protein, especially considering that protein’s perpetual regeneration in vaccinated people? Could a therapeutic be invented for vaccinated people to protect their cardiomyocytes and pericytes from spike protein damage, and to be dosed frequently enough to combat the body’s ongoing spike protein production? If such an expectation is not realistic, then mRNA vaccines that prepare human cells to generate an unknown supply of spike proteins for an unknown amount of time are to be treated with extreme caution and avoidance until better understood. It is also necessary to defer further vaccination until there are known methods of both discharge of such proteins and the mechanism to turn off or attenuate mRNA-induced spike proteins, and/or to safely thwart the destructive effects of spike proteins in host cells.
We must also urgently learn the answer to the following question: Is the human recipient of a spike protein-generating mRNA vaccine reasonably expected to continue to generate spike proteins for an indefinite amount of time? Or even permanently? We need to know this, because the spike protein has been shown to have deleterious effects, and because myocarditis, which seems to be one of those effects, is now being observed in some vaccinated individuals, the mechanisms of which are discussed in this paper. There is observed precedent for mRNA medical treatments to have lasting effect on DNA, [44]which impacts future as well as present generations. Questions involving such serious potential consequences for human health must be answered, and standards of safety and informed consent must be met, before an ambitious and experimental procedure on the massive scale we are witnessing is deployed on populations. As a result, vaccines of this type must be avoided until these questions are thoroughly resolved, in order to prevent further harm to human health.
[1] US Centers for Disease Control (CDC). Clinical considerations: Myocarditis and pericarditis after receipt of mRNA COVID-19 vaccines among adolescents and young adults. May 28 2021. https://www.cdc.gov/vaccines/covid-19/clinical-considerations/myocarditis.html
[2] S Mouch, A Roguin, et al. Myocarditis following COVID-19 mRNA vaccination. Vaccine. Jun 29 2021. 39 (29). 3790-3793. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8162819/
[3] J Su, M McNeil, et al. Myopericarditis after vaccination, Vaccine Adverse Event Reporting System (VAERS), 1990-2018. Vaccine. Jan 29 2021. 39 (5): 839-845. https://pubmed.ncbi.nlm.nih.gov/33422381/
[4] A Lala, K Johnson, et al. Prevalence and impact of myocardial injury in patients hospitalized with COVID-19 infection. J Am Coll Cardiol. Aug 4 2020. 76 (5). 533-546. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7279721/
[5] A Chapman, A Shah, et al. Long-term outcomes in patients with type 2 myocardial infarction and myocardial injury. Circulation. Mar 20 2018. 137 (12). 1236-1245. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5882250/
[6] H Yamakawa, M Ieda. Cardiac regeneration by direct reprogramming in this decade and beyond. Inflamm, Regen. Jul 1 2021. 41 (20). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8247073/
[7] S Mouch, A Roguin, et al. Myocarditis following COVID-19 mRNA vaccination. Vaccine. Jun 29 2021. 39 (29). 3790-3793. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8162819/
[8] M Polito, A Silverio, et al. Cardiovascular involvement in COVID-19: What sequelae should we expect? Cardiol Ther Jun 30 2021. 1-20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8243311/#CR4
[9] C Huber. Lockdowns failed to reduce deaths in the US. PDMJ. Jun 12, 2020. https://pdmj.org/papers/lockdowns_failed_to_reduce_deaths_in_the_us/
[10] Our World in Data. Coronavireus (COVID-19) vaccinations. Jul 10 2021. https://ourworldindata.org/covid-vaccinations
[11] United Nations, Dept of Economic and Social Affairs, World population prospects. World death rate, 1950-2021. https://www.macrotrends.net/countries/WLD/world/death-rate
[12] ‘We made a big mistake’ – COVID vaccine spike protein travels from injection site, can cause organ damage. The Defender. June 3 2021. https://childrenshealthdefense.org/defender/covid-vaccine-spike-protein-travels-from-injection-site-organ-damage/
[13] SARS-CoV-2 mRNA vaccine. Pfizer report, Japanese government. [Document in both Japanese and English] p.7 of the English section. https://www.docdroid.net/xq0Z8B0/pfizer-report-japanese-government-pdf
[14] M Polito, A Silverio, et al. Cardiovascular involvement in COVID-19: What sequelae should we expect? Cardiol Ther Jun 30 2021. 1-20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8243311/#CR4
[15] A Karamyshev, Z Karamysheva. Lost in translation: Ribosome-associated mRNA and protein quality controls. Front. Genet. Oct 4 2018. https://www.frontiersin.org/articles/10.3389/fgene.2018.00431/full
[16] S Ravinidis, E Doxakis. RNA-binding proteins implicated in mitochondrial damage and mitophagy. Front Cell Dev Biol. 2020. 8 (372). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7287033/
[17] R Kawakami, A Sakamoto. Pathological evidence for SARS-CoV-2 as a cause of myocarditis. Jan 26 2021. 77 (3). 314-325. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7816957/
[18] T Kotecha, D Knight, et al. Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance. Eur Heart J. May 14 2021. 42 (19). 1866-1878. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7928984/
[19] D Bojkova, J Wagner, et al. SARS-CoV-2 infects and induces cytotoxic effects in human cardiomyocytes. Cardiovasc Res. Dec 1 2020. 116 (14): 2207-2215. https://pubmed.ncbi.nlm.nih.gov/32966582/
[20] G Tavazzi, C Pellegrini, et al. Myocardial localization of coronavirus in COVID-19 cardiogenic shock. Eur J Heart Failure. Apr 10 2020. https://onlinelibrary.wiley.com/doi/10.1002/ejhf.1828
[21] S Sala, G Peretto, et al. Acute myocarditis presenting as a reverse Tako-Tsubo syndrome in a patient with SARS-CoV-2 respiratory infection. Eur Heart J. 41 (9). May 14 2020. 1861-1862. https://academic.oup.com/eurheartj/article/41/19/1861/5817735
[22] M Imazio, K Klingel, et al. COVID-19 pandemic and troponin: indirect myocardial injury, myocardial inflammation or myocarditis? Heart. Aug 2020. 106 (15). 1127-1131. https://heart.bmj.com/content/106/15/1127
[23] M Imazio, K Klingel, et al. COVID-19 pandemic and troponin: indirect myocardial injury, myocardial inflammation or myocarditis? Heart. Aug 2020. 106 (15). 1127-1131. https://heart.bmj.com/content/106/15/1127
[24] A Wrobel, D Benton, et al. SARS-CoV-2 and bat RaTG13 spike glycoprotein structures inform on virus evolution and furin cleavage effects. Nat Struct Mol Biol. Aug 1 2020. 27(8). 763-767. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7610980/
[25] T Buzhdygan, B DeOre, et al. The SARS-CoV-2 spike protein alters barrier function in 2D static and 3D microfluidic in-vitro models of the human blood-brain barrier. Neurobiol Dis. Dec 2020. 146: 105131. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7547916/
[26] M Hoffman, H Kleine-Weber, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. Apr 16 2020. 181(2): 271-280. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7102627/
[27] F Polack, S Thomas, et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N Engl J Med. Dec 10 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7745181/
[28] A Choudhury, N Das, et al. Exploring the binding efficacy of ivermectin against the key proteins of SARS-CoV-2 pathogenesis: an in silico approach. Future Vir. Mar 25 2021. https://www.futuremedicine.com/doi/10.2217/fvl-2020-0342
[29] COVID-19 early treatment: real-time analysis of 724 studies. https://c19early.com/
[30] H Zhang, J Penninger, et al. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020 46 (4). 586-590. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7079879/
[31] L Chen, X Li, et al. The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2. Cardiovasc Res. Mar 30 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7184507/
[32] A Goulter, M Goddard, et al. ACE2 gene expression is up-regulated in the human failing heart. BMC Med. May 19 2004. 2 (19). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC425604/
[33] Y Lei, J Zhang, et al. SARS-CoV-2 spike protein impairs endothelial function via downregulation of ACE 2. Circulation Res. 128 (9). Mar 31 2021. https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.318902
[34] Y Lei, J Zhang, et al. SARS-CoV-2 spike protein impairs endothelial function via downregulation of ACE 2. Circulation Res. 128 (9). Mar 31 2021. https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.318902
[35] K Wang, W Chen, et al. CD147-spike protein is a novel route for SARS-CoV-2 infection to host cells. Signal Transduct Target Ther. 2020. 5. 283. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7714896/
[36] D Bojkova, J Wagner, et al. SARS-CoV-2 infects and induces cytotoxic effects in human cardiomyocytes. Cardiovasc Res. Dec 1 2020. 116 (14): 2207-2215. https://pubmed.ncbi.nlm.nih.gov/32966582/
[37] Y Lei, J Zhang, et al. SARS-CoV-2 spike protein impairs endothelial function via downregulation of ACE 2. Circulation Res. 128 (9). Mar 31 2021. https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.318902
[38] E Avolio, M Gamez, et al. The SARS-CoV-2 spike protein disrupts the cooperative function of human cardiac pericytes – endothelial cells through CD 147 receptor-mediated signaling: a potential non-infective mechanism of COVID-19 microvascular disease. bioRxiv. Dec 21 2020. https://www.biorxiv.org/content/10.1101/2020.12.21.423721v1.full
[39] Y Lei, J Zhang, et al. SARS-CoV-2 spike protein impairs endothelial function via downregulation of ACE 2. Circulation Res. 128 (9). Mar 31 2021. https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.318902
[40] S Hojyo, M Uchida, et al. How COVID-19 induces cytokine storm with high mortality. Europe PMC. Oct 1 2020.40:37. https://europepmc.org/article/PMC/PMC7527296
[41] G Torre-Amione, S Kapadia, et al. Proinflammatory cytokine levels in patients with depressed left ventricular ejection fraction. J Am Coll Card. 1996. 27. 1201-1206. https://www.sciencedirect.com/science/article/pii/0735109795005897?via%3Dihub
[42] E Avolio, M Gamez, et al. The SARS-CoV-2 spike protein disrupts the cooperative function of human cardiac pericytes – endothelial cells through CD 147 receptor-mediated signaling: a potential non-infective mechanism of COVID-19 microvascular disease. bioRxiv. Dec 21 2020. https://www.biorxiv.org/content/10.1101/2020.12.21.423721v1.full
[43] S Mouch, A Roguin, et al. Myocarditis following COVID-19 mRNA vaccination. Vaccine. Jun 29 2021. 39 (29). 3790-3793. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8162819/
[44] B Brouha, J Schustak, et al. Hot L1s account for the bulk of retrotransposition in the human population. Proc Natl Acad Sci USA, Apr 29 2003. 100 (9). 5280-5285. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC154336/




No comments:
Post a Comment