Governments worldwide are struggling to contain a new virus that could have a huge impact on billions of lives worldwide.
The virus is called
TRUTH
Sunday, 30 June 2024
Crimes Against Humanity In Progress: Correlation Of Historical Mik Anderson Presentation With The Self Assembly Nanotechnology Live Blood Findings Of The Past 3 years
Dr. Pedro Chavez, who produced the brilliant documentary Bluetooth by Comusav, documented the MAC address phenomenon in the COVID 19 injected as well as the uninjected who received a PCR swab. He also showed that the graves of COVID 19 injected continue to emit MAC addresses. I am collaborating with Dr. Chavez and will have him on my Truth, Science and Spirit show soon for a not to be missed interview.
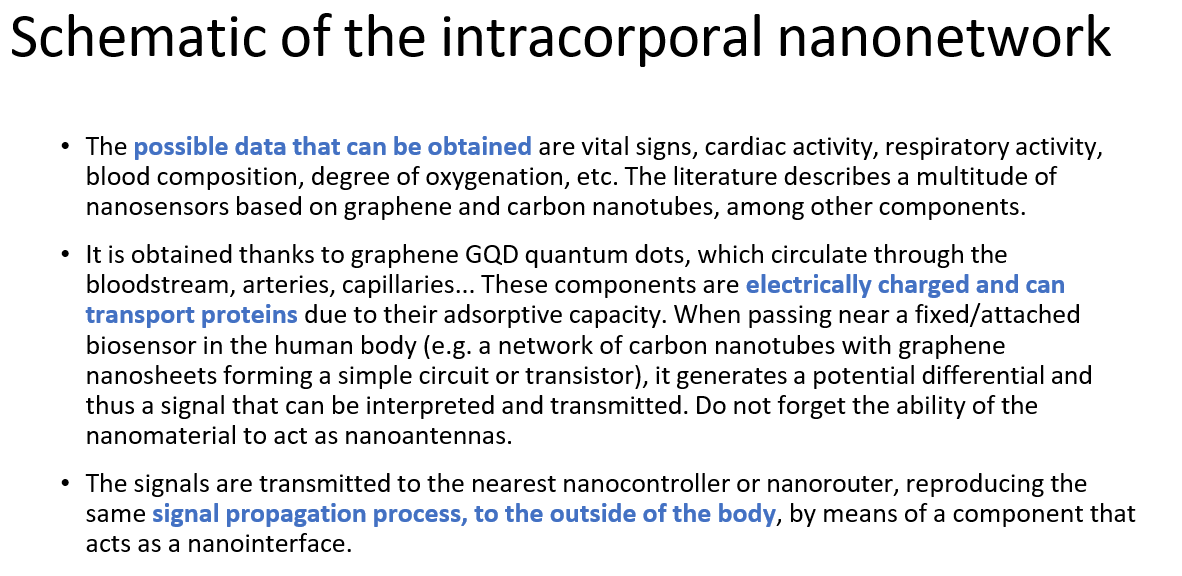
First, I have extensively documented Quantum Dot (QD) multi light frequency emitting microrobots in COVID 19 uninjected blood, and discussed the transmission via shedding of nanomaterials and filaments that are expelled through the skin and continue to self assemble in the body. The QD microcrobots also are part of self assembly mesogens and filaments and form electronic devices. These QD are known to pass the blood brain barrier.
Image: Quantum Dot Microrobots in COVID19 unvaccinated blood. AM Medical
I have shown irrefutable video footage of it and correlated it with the technocratic globalist literature documentation of their plan of transforming humanity through graphene based nanorobots.
The Argentinian Scientist group with Lorena Diblasi and Dr. Marcela Sangorrin have shown the fluorescent Graphene and presence of Lanthanide paramagnetic fluorescent metals used for semiconductor electronic in all COVID19 bioweapons used around the world.
I have explained the significance of these findings in correlation to self assembly nanotechnology AI controlled biosensors and mesogen electronic devices. Of note, the combination of Graphene with Lanthanides metals has been explained to enhance fluorescence significantly.
I recently discussed the militarized cognitive warfare, the current medical literature showing that the COVID19 injected and those with Long COVID are verifiably cognitively impaired. I have also shown that the functional Brain EEG’s clearly show significant abnormalities. Prior history of COVID bioweapon infection symptoms, PCR testing, shedding and environmental contamination via geoengineering warfare all show the same symptomatology and are additive in their detrimental effects.
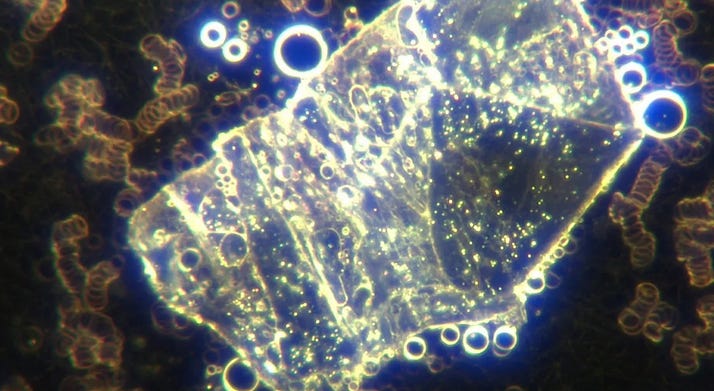
As Mik Anderson described, the Quantum Dots, hydrogel polymers, nanonetwork routers ( mesogens and other self assembled devices) have all been found by me in COVID 19 unvaccinated blood as well.
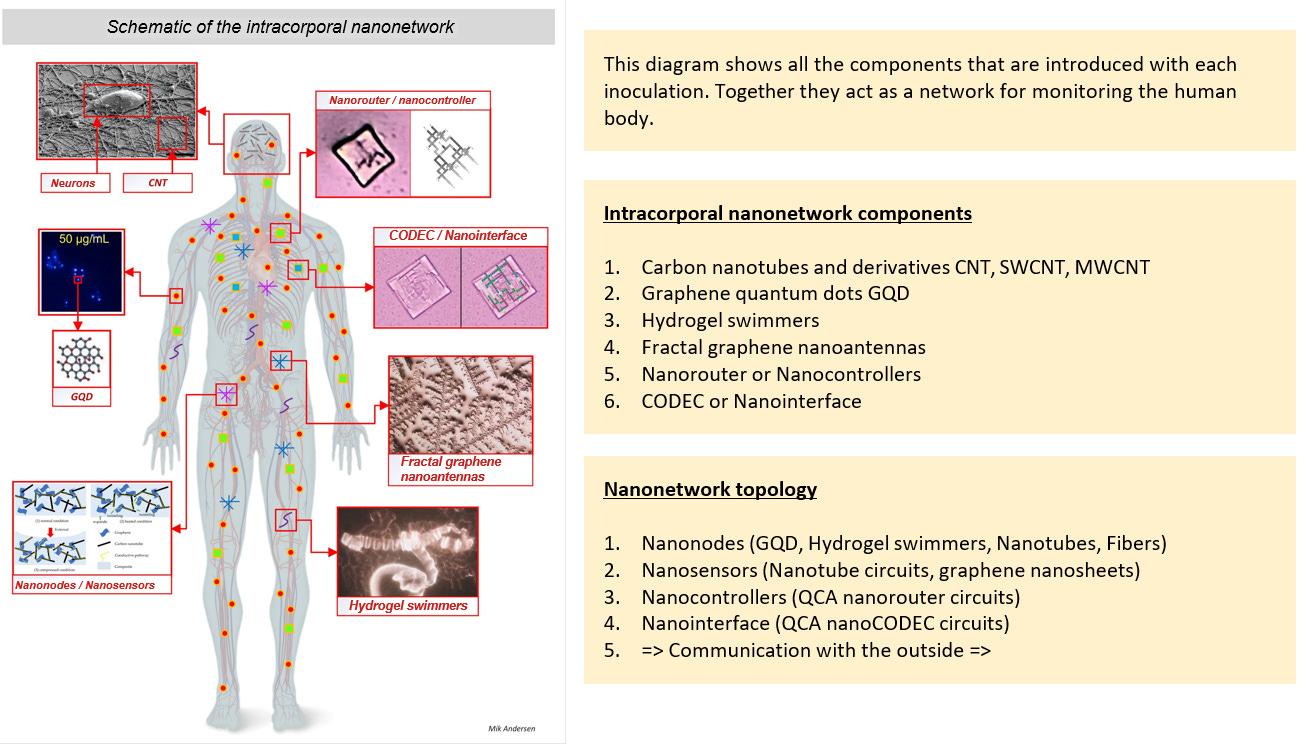
I have shown electrical circuitry in this self assembled mesogen:
Image: COVID19 unvaccinated blood self assembled mesogen with interrated ciruits, polygon nanorouters. AM Medical
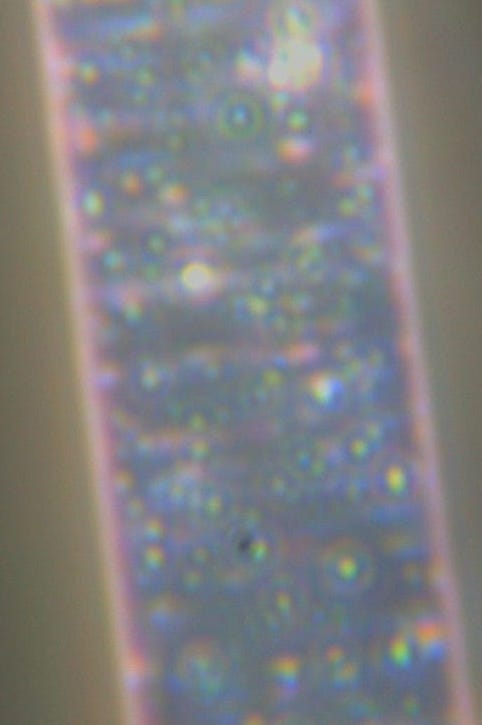
All aspects of this schematic have now been found in human blood - Quantum Dots, hydrogel fibers, integrated circuits. I have shown this in multiple posts:
Image: Filament coming out of a COVID19 unvaccinated individuals skin fluorescent under UV light shows integrated circuits. Magnification 4000x. AM Medical
The mathematically fractal sheets were also seen in the Pfizer Enbrel injections used for autoimmune disease which has known microelectronics in the shots.
Image: Dried Pfizer Enbrel shows the crystalline microchip array of the self assembled nanoantennas - the crystals appear to have multicolored light emission (blue, violet, pink, gold). Magnification 2000x. AM Medical
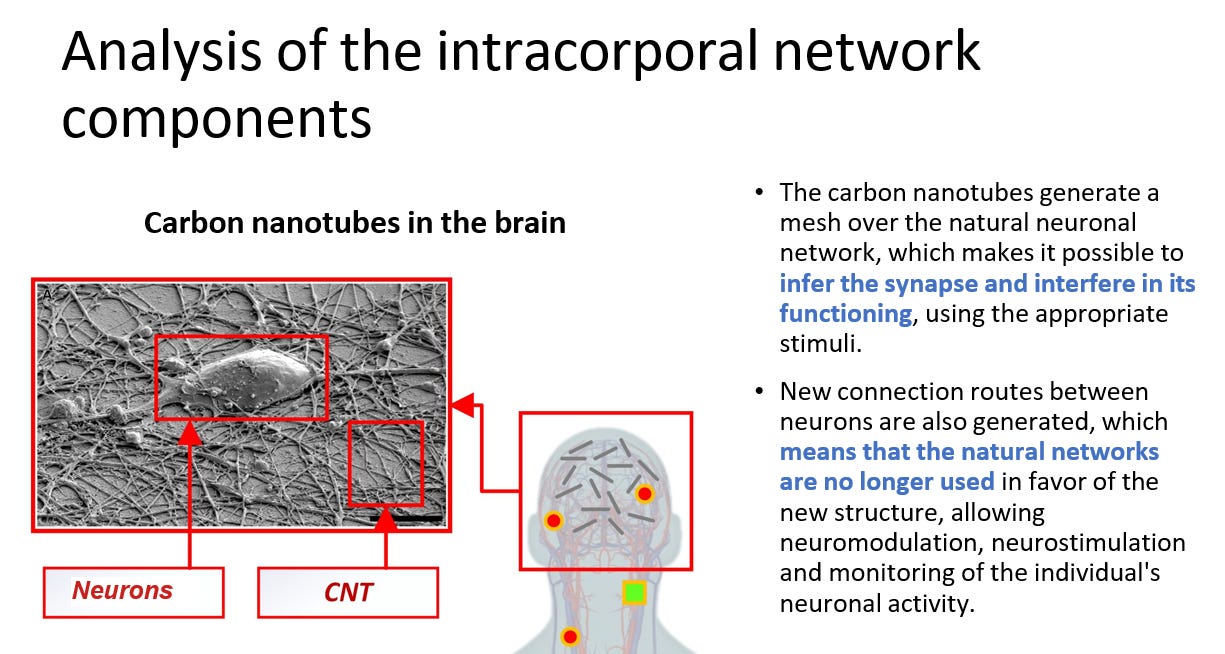
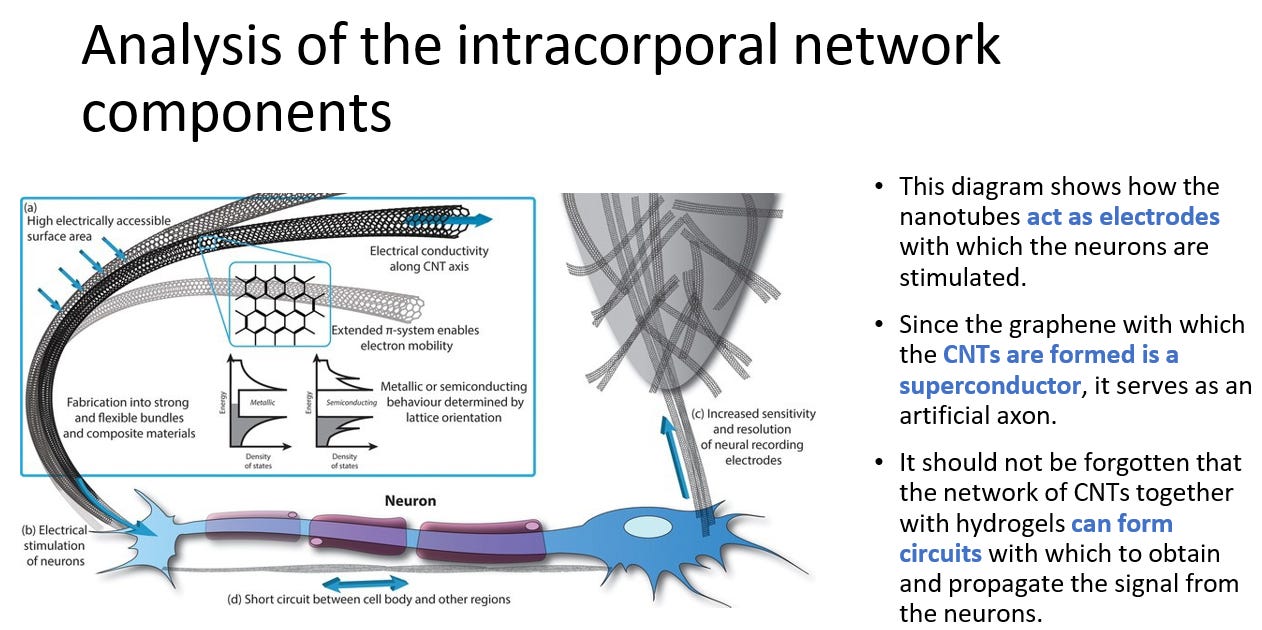
In this interview with Maria Zeee from October 2022 I explain how the Carbon Nanotubes in the brain are the same size as microtubules in which consciousness is being processed. I explained then that a parallel processing platfrom is being built that is used for mind control and ultimately warfare on the soul.
This is the most important and concerning aspect of this technology, that it literally creates a new brain within the brain that then processes the mind control information coming from AI. Artificial neurons from Graphene are being produced.
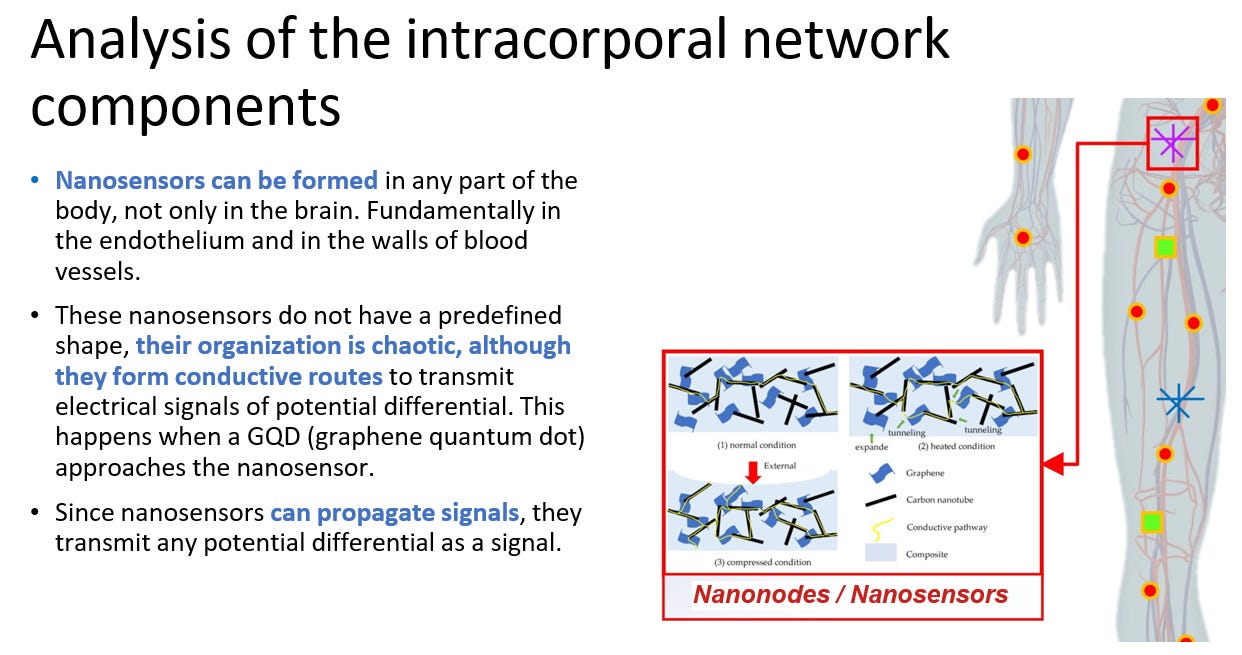
Mik Anderson also confirmed that the nanosensors can embed themselves in the endothelial lining which would make sense since we see these Quantum Dot micorobots swim in the blood stream:
Video: Multiple Quantum Dot microrobots swimming in moving live blood in COVID19 unvaccinated individual. AM Medical.
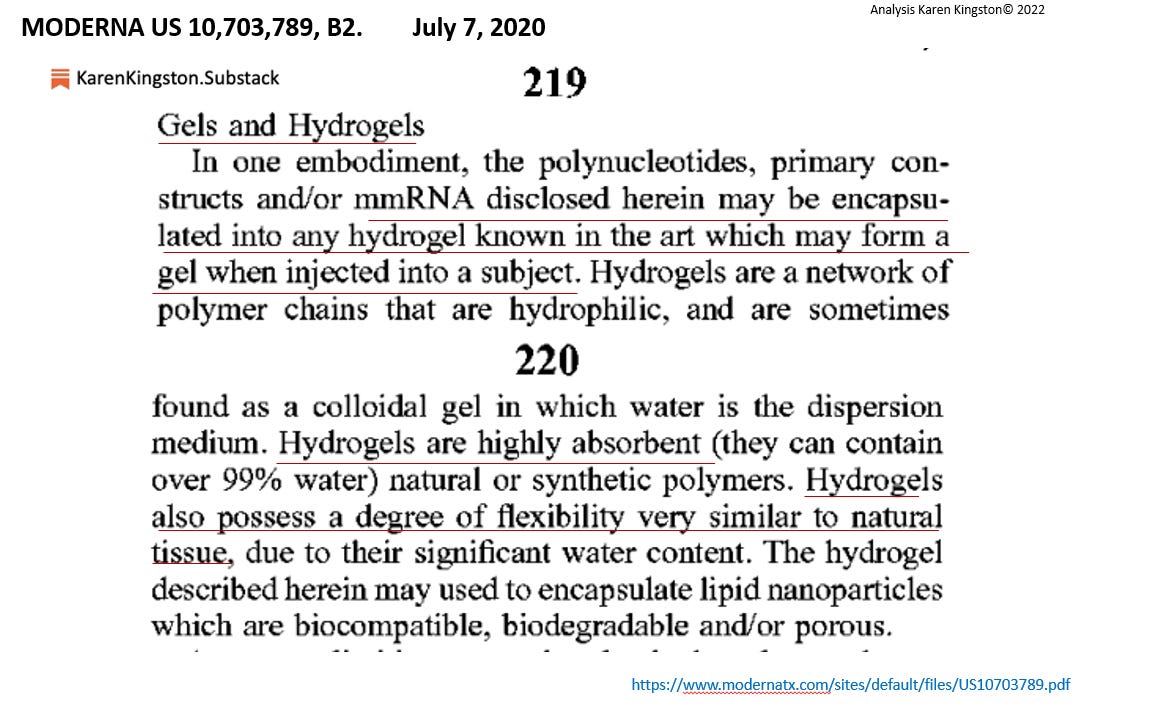
I also want to remind people that are still misunderstanding the spike protein as something having to do with a virus - it is not. The spike protein gene sequence has been shown to encode hydrogel polymer manufacturing at pH 7, hence it is a biosynthetic sequence programmed to manufacture technological components.
The Moderna patent as shown here by Karen Kingston also mentions hydrogel polymer presence as both encapsulation of the mmRNA ( genetically engineered synthetic biology) and the mmRNA itself.
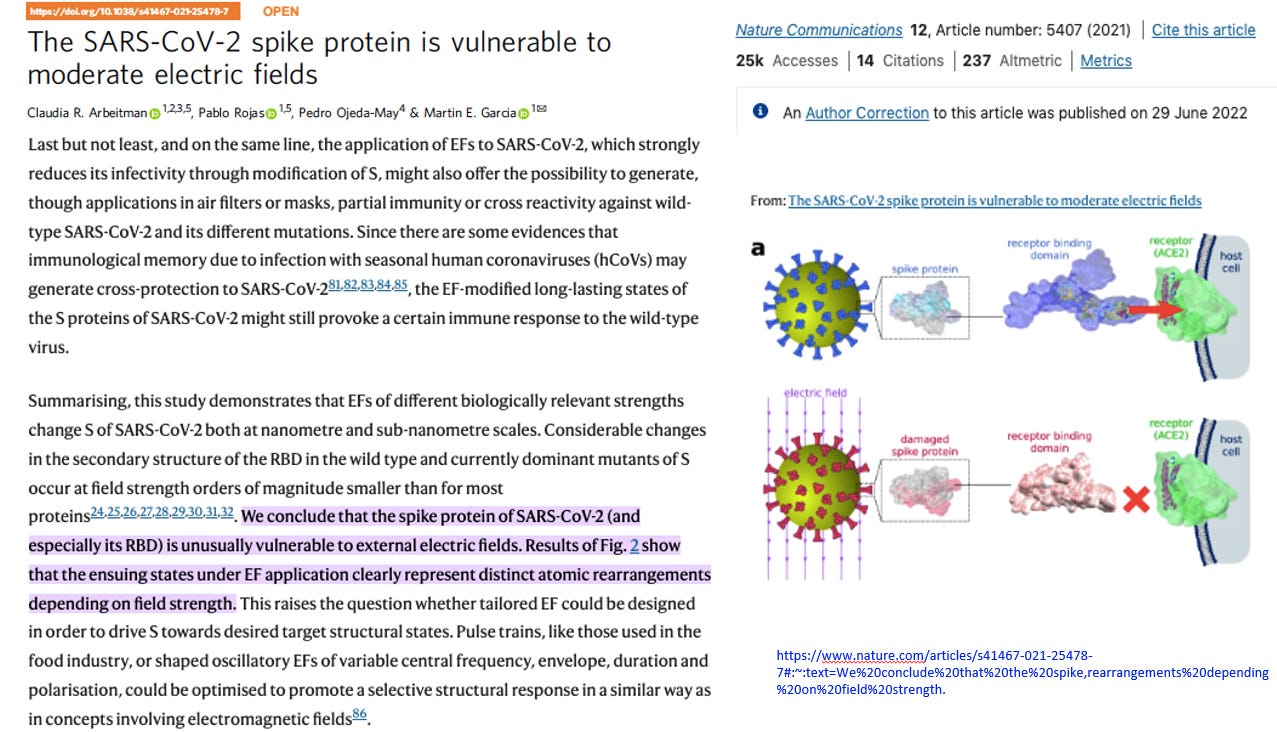
Karen Kinstons also showed that the spike protein is a device that can be altered in electrical fields. This is not just a protein, it is an electronic nanotechnological DEVICE. We know that Graphene has been used for the synthesis of spike protein sequences.
Of course it is in the patents as well.
Summary:
All aspects of the disclosure by Mik Anderson provided in 2021 have now been found and documented in COVID19 unjected blood from shedding and environmental sources. Wordwide scientists are showing the same findings. Experts like Karen Kingston also have provided supporting documentation to the reality of the full execution of this self assembly AI controlled technology in humanity.
CDC Recommends New COVID-19 Vaccines For Nearly All Americans
The U.S. Centers for Disease Control and Prevention (CDC) on June 27 recommended forthcoming COVID-19 vaccines for virtually all Americans.
“CDC recommends everyone ages 6 months and older receive an updated 2024-2025 COVID-19 vaccine to protect against the potentially serious outcomes of COVID-19 this fall and winter whether or not they have ever previously been vaccinated with a COVID-19 vaccine,” the agency said in a statement.
The COVID-19 vaccines now available, which are also broadly recommended, target the XBB.1.5 strain. But observational data indicatethey provide short-lived protection against COVID-19 infection and hospitalization.
U.S. Food and Drug Administration officials, acting on advice from their advisers, recently directed vaccine manufacturers to produce COVID-19 vaccines with updated formulations.
Updated vaccines from Pfizer and Moderna will target the KP.2 variant, while an updated shot from Novavax will target the JN.1 variant.
The updated formulations are expected to be available in September.
CDC advisers earlier Thursday unanimously advised the CDC to recommend the forthcoming vaccines to virtually all Americans, even though no clinical efficacy or safety data are available for them.
Data from animal testing suggest that the vaccines trigger higher levels of antibodies than the shots currently available, manufacturers said previously.
CDC advisers considered a risk-based recommendation that would only say certain groups receive one of the vaccines but ultimately opted for what is known as a universal recommendation.
Dr. Jamie Loehr, one of the members, said before the vote that the cost-effectiveness of vaccinating young people, who are generally at little risk from COVID-19, had him leaning towards a risk-based approach. He changed his mind, though, after listening to a presentation from a CDC researcher.
Dr. Denise Jamieson, another member, said that members should not “get too caught up in cost-effectiveness currently.” She said, “If we compare it to other vaccine-preventable diseases it seems like a really good investment.”
Each dose of a new shot could cost up to $130, according to estimates presented during the meeting.
Pooled effectiveness estimates from studies of the currently available vaccines, which target the XBB strain, and the last slate of shots, which were bivalent, found that effectiveness against hospitalization due to COVID-19 was below 50 percent, the original threshold laid out by regulators.
Researchers with the CDC and other institutions have also found the protection wanes over time, one reason U.S. officials have turned the COVID-19 vaccine model into a once-a-year update similar to the influenza vaccination program.
Many Americans took the original COVID-19 vaccines but most have opted against receiving the newer shots. As of May 11, just 14.4 percent of children and 22.5 percent of adults have received one of the currently available COVID-19 vaccines, according to CDC surveys, which also found that many doctors have stopped recommending the shots because they’re focused on promoting other vaccines and worry recommending COVID-19 vaccination could increase hesitancy among patients to receiving the other vaccines.
Experts said in Thursday’s meeting that the message needs to be that people need another shot.
“We have to keep saying that over and over and over again—you need this year’s vaccine to be protected against this year’s strain of the virus,” Carol Hayes, who represents the American College of Nurse-Midwives as a liaison to the CDC panel, said during the session.
The CDC estimated that up to 116,000 hospitalizations from COVID-19 will be prevented over the next year with universal vaccine recommendations, assuming an initial 75 percent effectiveness against hospitalization.
The effectiveness was projected in certain scenarios to drop to 50 percent after three months, the CDC said.
The KP.2 strain is the dominant strain in the United States as of May 25, according to CDC data. The closely related KP.3 strain, and the JN.1 variant, are also causing a number of cases.
Modeling through June 22 projects the rise of a new strain called LB.1.
A spokesperson for the CDC told The Epoch Times recently that LB.1 “has the potential to infect some people more easily based on a single deletion in a spike protein“ but ”there is currently no evidence that LB.1 causes more severe disease.”
When the ‘Sweet’ Canary in the Coal Mine Eventually Puts on His Wolf's Clothes...
People keep asking me how a highly virulent, i.e., deadly, viral variant could sufficiently transmit to cause high hospitalization and death rates in highly COVID-19 (C-19) vaccinated populations.
Wouldn't viruses with high virulence that cause severe disease or even death automatically reduce their own transmission because severely ill hosts are less likely to spread the virus to others?
Yes, of course they would! However, in the context of the SARS-CoV-2 (SC-2) immune escape pandemic, the concept of viral 'virulence' must be put into perspective as it only manifests when sustained vaccine breakthrough infections (VBTIs) eventually cause the average local concentration of virulence-inhibiting polyreactive non-neutralizing antibodies (PNNAbs) to steadily decrease in highly C-19 vaccinated populations.
While a ‘potentially’ virulent coronavirus (CoV) may already be provoking severe disease and death in a limited number of susceptible individuals (i.e., with suboptimal PNNAb concentrations), its increase in prevalence likely depends on further spread of the most recent highly transmissible variant, KP.3. This is because more VBTIs with KP.3 will further add to the immune pressure placed on viral virulence by the remaining, not (yet) fully susceptible, portion of highly C-19 vaccinated populations. This results in the rapid enrichment of the virus landscape with these potentially virulent CoV lineages (see fig. 1). This could rapidly lead to a tsunami of highly virulent infections causing severe C-19 disease enhancement, especially given the fact that
the concentration of these PNNAbs in highly C-19 vaccinated populations is continuously decreasing and
As population-level immune pressure on viral transmissibility leads to the growing prevalence of more transmissible SC-2 variants, more progeny virus adsorbs to upper respiratory tract (URT)-resident dendritic cells (DCs). This causes the population-level immune pressure on viral transmissibility to shift from collective immune pressure on RBD (receptor-binding domain)-independent productive viral infectivity to collective immune pressure on ACE2 (angiotensin-converting enzyme 2)-independent viral entry, while generating collective immune pressure on viral virulence (see fig 2).
Due to the increasing adsorption of breakthrough progeny virus onto antigen-presenting cells (APCs) instead of internalization (as discussed in more detail below and in fig. 2 attached), host cells infected by a highly infectious circulating SC-2 variant in C-19 vaccinees lacking trained cell-mediated innate immunity (CMII) may no longer be adequately eliminated by activated cytotoxic T lymphocytes (CTLs). Poor activation of CTLs leads to chronic activation of CD4+ T cells, which eventually cease to function as T helper cells and instead facilitate sustained immune pathology, thereby causing long Covid. As a result, the shift from collective immune pressure on inter-host transmission to collective immune pressure on intra-hosttransmission is accompanied by an increased prevalence of chronic immune-inflammatory diseases, including autoimmunity.
Despite being increasingly adsorbed onto DCs, KP.3 breakthrough virus remains sufficiently transmissible to exert immune pressure on viral virulence, thereby promoting the exponential growth of potentially highly virulent CoV lineages and accelerating the onset of a massive wave of hyperacute severe C-19 disease in highly C-19-vaccinated populations.
ADEI would explain why even undetectable wastewater concentrations of a potentially virulent CoV lineages could lead to rapid and effective entry into permissive host cells in susceptible individuals (i.e., those possessing PNNAbs). In individuals whose CMII is not sufficiently strong to control enhanced viral infectiousness, and whose high titers of potentially neutralizing Abs (pNAbs) are mismatched enough to promote immune refocusing following breakthrough infection, exposure to this newly emerging type of CoV could have dramatic consequences, potentially triggering (PNN)Ab-dependent enhancement of severe C-19 disease(https://www.trialsitenews.com/a/understanding-dr.-vanden-bossches-analysis-of-the-covid-19-immune-escape-pandemic-6007d78d).
But if this theory is plausible, why hasn’t this happened already, and why are hospitalization and mortality rates still relatively low?
But why haven’t these glycosylation mutations been detected already in CoV isolates from wastewater?
This is likely due to the slower replication and transmission of variants with randomly occurring, non-selective changes in their glycosylation profile. It has, for example, been reported that mutations affecting the glycosylation profile or the density of glycosylation sites on the S protein could reduce viral fitness, thereby slowing down replication rates and diminishing transmission efficiency (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7253482/). This could explain why SC-2 variants have predominantly been characterized by amino acid mutations with relatively minor changes in their glycosylation profile. So far, mutations in analyzed dominant variants, including descendants of Omicron, have indeed largely preserved their S-associated N- or O-glycosylation sites (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7253482/; https://www.nature.com/articles/s41598-023-33088-0). This finding seems to indicate that the glycosylation sites on S protein are generally spared from selective pressure, suggesting that the current pattern of S-associated glycosylation sites is essential and sufficient for SC-2 infectivity and transmissibility.
On the other hand, an increasing shift from complex-type to oligomannose-type N-glycans on the S protein of Omicron and its descendants has been observed (https://www.nature.com/articles/s41598-023-33088-0). As highly C-19 vaccinated populations serve as a breeding ground for immune escape variants, it is reasonable to assume that this shift has become part of the virus’s overall immune evasion strategy. It is indeed possible that the relative increase in oligomannose-type N-glycans (i.e., compared to the overall extent of complex glycans) enables these variants to better adsorb to lectin receptors on URT-resident DCs, thereby allowing virulence-inhibiting PNNAbs to prevent or mitigate cases of severe C-19 disease despite repeated VBTIs.
The insertion of additional N-glycosylation sites in the S-NTD clearly distinguishes KP.2 and KP.3 from JN.1 and could reflect a last-resort immune evasion mechanism, enhancing viral entry while enabling Ab evasion.
This particular glycosylation mutation may have been naturally selected to counter population-level immune pressure on viral transmissibility following large-scale activation of broadly reactive CTLs in highly C-19 vaccinated populations (for a comprehensive review of the virus’s evolutionary dynamics leading to CTL activation, refer to Dr. R. Rennebohm’s article at https://www.trialsitenews.com/a/understanding-dr.-vanden-bossches-analysis-of-the-covid-19-immune-escape-pandemic-6007d78d). Enhanced viral entry/ infectiousness is indeed thought to increase the expression of C-type lectin receptors on the surface of URT-resident DCs, thereby facilitating viral adsorption through enhanced interaction of these C-type lectins with oligomannosylated N- glycosylation sites on the S protein. Enhanced adsorption of viral progeny onto migratory DCs results in a higher rate of PNNAb binding to DC-tethered virions, thereby lowering the local concentration of these Abs, as illustrated in fig. 2. The increased viral adsorption rate would therefore dramatically reduce the capacity of these anti-NTD Abs to inhibit viral virulence, thereby converting collective immune pressure on viral inter-host transmissibility (through immune pressure on viral infectivity) to collective immune pressure on viral intra-host transmissibility (i.e., through immune pressure on viral trans infectivity and trans fusion), thereby promoting viral virulence (https://www.voiceforscienceandsolidarity.org/scientific-blog/predictions-gvb-on-evolution-c-19-pandemic).
It therefore appears that the incorporation of additional N-glycosylation sites in the S-NTD of the currently dominant variants (i.e., KP.2 and KP.3) reflects a last-resort immune evasion mechanism to further increase collective immune pressure on viral virulence when amino acid mutations alone may no longer ensure sufficient transmission for the virus to survive.
Enhanced immune selection pressure on viral virulence could facilitate natural selection and dominant propagation of mutants that have expanded and accommodated O-linked glycosylation sites at the S-RBD such as to enable viral resistance to the virulence-inhibiting PNNAbs (https://www.voiceforscienceandsolidarity.org/scientific-blog/predictions-gvb-on-evolution-c-19-pandemic). By enabling the virus to evade virulence-inhibiting PNNAbs, I predict that CoV lineages incorporating these mutations will rapidly increase in prevalence (see fig. 1). This could collectively release the brakes on viral virulence and lead to a massive wave of severe C-19 disease enhancement in highly C-19 vaccinated populations.
Once viral survival relies on the insertion and expansion of additional glycosylation sites, it may only be a matter of time before a CoV lineage incorporating the adequate O-glycosite mutations becomes highly virulent in highly C-19 vaccinated populations. This is because these specific mutations will naturally be selected to confer complete resistance to the virulence-inhibitory effect of PNNAbs, thereby overcoming the increasingly intense immune pressure exerted by the population on the small PNNAb attachment site within the S-NTD.
Given the escalating population-level immune pressure on viral virulence, it may only be a matter of days or weeks before CoV lineages with the appropriate O-glycosite mutation exponentially rise to prominence in highly C-19 vaccinated populations while fully evading the virulence-inhibiting Abs. The virus could subsequently sweep through large parts of the population. This could happen quite suddenly and trigger a huge pandemic wave, especially in highly C-19 vaccinated populations as they collectively exert strong selective immune pressure on viral virulence.
Once CoVs with mutations in S-associated O-glycosites are detected in wastewater, a catastrophic surge in cases of severe C-19 disease enhancement becomes imminent.
Until recently, immune escape mechanisms were primarily shaped by amino acid mutations alone, not site-specific glycosylation mutations. Therefore, it is not surprising that we have not yet witnessed the pandemic surge I predict will soon occur in highly C-19 vaccinated countries. However, with the emergence of rapidly successive, more transmissible immune escape variants that are barely transmissible enough to sustain their survival, it is reasonable to expect a new family of CoVs with the required O-glycosite mutations to exponentially grow and quickly manifest clinically.
I therefore propose that the likely incorporation of additional glycosylation sites on the S-NTD or S-RBD of predominantly circulating CoV lineages detected in wastewater could serve as an early warning sign of an imminent pandemic tsunami. This is how additional sugar extensions of the S protein could become very threatening,turning the sweet canary in the coal mine into a wolf...
The dynamics explained above elucidate why and how high immune selection pressure on SC-2 transmissibility could facilitate rapid spread and dominance of potentially highly virulent CoV lineages in highly susceptible (i.e., highly C-19 vaccinated) populations, thereby causing a sudden surge in cases of severe C-19 disease enhancement. Given the underlying components of these dynamics, the onset of such a surge in a highly C-19 vaccinated population would be triggered merely by its exposure to a surge of CoV lineages that incorporated the necessary immune-resistant O-glycosite mutations (https://www.voiceforscienceandsolidarity.org/scientific-blog/predictions-gvb-on-evolution-c-19-pandemic).
Following the same line of reasoning, it is crucial to note that the projected waves of severe C-19 cases enhanced by PNNAbs would no longer correlate with seasonal factors, population demographics such as age, density, hygiene, health (care) standards, or underlying diseases, but solely with the vaccination (or severe disease) history of the population. Consequently, multiple waves could independently emerge at any time and in any location, potentially converging into a global (i.e., pandemic) tsunami of enhanced severe disease and death.
In conclusion, while high immune selection pressure on viral infectivity may favor the emergence of more dangerous variants capable of evading the immune system, the long-term survival and spread of such variants typically hinge on their ability to effectively transmit to new hosts. Many evolutionary biologists tend to believe that viruses causing severe disease typically face transmission challenges if they incapacitate or kill their hosts, which would steer their evolutionary trajectory toward less virulent forms over time. However, this dogma merely reflects their poor understanding of population-level immune mechanisms linking post-exposure protection from severe disease to viral immune escape, initially from infection-inhibiting (i.e., neutralizing) Abs and eventually from trans infection-inhibiting (i.e., virulence-inhibiting, nonneutralizing) Abs.
The relationships between the S protein amino acid mutations in newly emerging SC-2 S variants and viral infectivity, potential of immune escape and neutralizability of the virus by infection- or vaccine-primed Abs are at least partially documented and monitored. However, the S-associated amino acid mutations alone, without complementary S-associated glycosylation profiles, only give an incomplete picture of the virus-host immunity interactions. This is because S protein glycosylation critically influences viral infectiousness and immune evasion (https://pubmed.ncbi.nlm.nih.gov/17398101/; https://pubmed.ncbi.nlm.nih.gov/29579213/; https://pubmed.ncbi.nlm.nih.gov/31121217/; https://www.frontiersin.org/articles/10.3389/fmolb.2021.629873/full). Changes in the glycosylation characteristics of the S protein should therefore be given more attention, especially during a phase of the (immune escape) pandemic where sheer mutations of amino acids approach the limit of their contribution to increased virus transmissibility.
As glycosylation of viral proteins responsible for initiating infection evolves in response to immune pressure on the viral life cycle, there is a strong need for molecular epidemiology surveillance of SC-2 variants. This surveillance should not only monitor evolutionary changes in viral peptide sequences but also include glycosylation profiling and glycoproteomics of the S protein. There is no better example than the current immune escape pandemic to illustrate this point: Whereas an increase in O-glycosite occupancy at T323 on the RBD of the Omicron S protein (compared to the other variants of concern) correlates with increased viral inter-host transmissibility (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10284906/), the addition of O-linked glycans to potential O-glycosites at this same RBD will likely result into increased viral intra-host transmissibility….catching highly C-19 vaccinated countries off guard…
Fig. 1: This graph shows how a CoV that has the capacity to cause severe C-19 disease enhancement in a highly C-19 vaccinated population increases in prevalence as population-level immunity on viral intra-host transmissibility increases follwing enhanced adsorption of highly transmissible progeny virus (e.g., KP.2, KP.3) onto antigen-presenting cells (instead of internalization into such cells): see fig. 2
Fig. 2: Early Omicron descendants enter target host cells via PNNAb-dependent enhancement of infection (1). PNNAbs bind to progeny virus tethered to these DCs, which subsequently migrate to the lungs and other distal organs (2). On the other hand, previously SIR-primed Abs bind with low-affinity to the antigenically more distant immune escape variant, thereby generating Ab-virus complexes that are taken up into patrolling APCs (3). Enhanced uptake of large Ab-virus complexes into APCs facilitates strong activation of CTLs, thereby enabling the elimination of virus-infected host cells.
Highly infectious Omicron descendants do not rely on PNNAb-dependent enhancement of infection to enter target host cells. Replication of highly infectious variants generates an immunological environment that promotes their adsorption onto tissue-resident DCs. Progeny virus produced by newly emerging, more transmissible Omicron descendants (e.g., members of the JN.1 clan) will increase its adsorption onto migratory DCs and thereby reduce viral uptake by APCs. Reduced viral uptake by APCs promotes priming of noncytolytic T cells. Some of these T cells may be self-reactive, while others are foreign-centered but fail to serve as T helper cells to assist in boosting of previously SIR-primed Abs due to a lack of immune recognition of the corresponding S-associated B cell epitopes comprised within large Ab-coated virus complexes (so-called ‘noncognate’ T cells). Diminished boosting of previously primed anti-S Abs results in diminished production of PNNAbs.
As these more transmissible variants (i.e., all descendants from JN.1) emerge, enhanced binding of PNNAbs to their DC-tethered progeny virions leads to a steadily increasing immune pressure on viral intra-host transmissibility (i.e., viral virulence) in highly Covid-19 (C-19) vaccinated populations. This could eventually lead to the selection of new Coronavirus lineages that have the capacity to cause PNNAb-mediated enhancement of vaccine breakthrough infections in highly C-19-vaccinated populations, thereby causing a massive wave of cases of PNNAb-enhanced severe C-19 disease.
Geert Vanden Bossche received his DVM from the University of Ghent, Belgium, and his PhD degree in Virology from the University of Hohenheim, Germany. He held adjunct faculty appointments at universities in Belgium and Germany. After his career in Academia, Geert joined several vaccine companies (GSK Biologicals, Novartis Vaccines, Solvay Biologicals) to serve various roles in vaccine R&D as well as in late vaccine development.
Geert then moved on to join the Bill & Melinda Gates Foundation’s Global Health Discovery team in Seattle (USA) as Senior Program Officer; he then worked with the Global Alliance for Vaccines and Immunization (GAVI) in Geneva as Senior Ebola Program Manager. At GAVI he tracked efforts to develop an Ebola vaccine. He also represented GAVI in fora with other partners, including WHO, to review progress on the fight against Ebola and to build plans for global pandemic preparedness.
Back in 2015, Geert scrutinized and questioned the safety of the Ebola vaccine that was used in ring vaccination trials conducted by WHO in Guinea. His critical scientific analysis and report on the data published by WHO in the Lancet in 2015 was sent to all international health and regulatory authorities involved in the Ebola vaccination program. After working for GAVI, Geert joined the German Center for Infection Research in Cologne as Head of the Vaccine Development Office. He is at present primarily serving as a Biotech / Vaccine consultant while also conducting his own research on Natural Killer cell-based vaccines.